Eunuch, in the etymological sense, is derived from the Greek words “eune,” meaning “bed,” and “ekho,” meaning protector/keeper. Eunuchoidism refers to a disorder of male gonadal insufficiency noted after castration.
This state of androgenic failure results in various eunuchoid body shapes, depending on the timing of androgen withdrawal – congenital, peripubertal, or post-pubertal.
Classification of eunuchoid body habitus
Timing of castration (androgen withdrawal) and eunuchoid body shape or habitus
| Timing of castration | Clinical features |
| Congenital/Early in life | Broad pelvis |
| Peripubertal | Broad pelvis and Narrow shoulders |
| Postpubertal | Narrow pelvis and Broad Shoulders of a normal male |
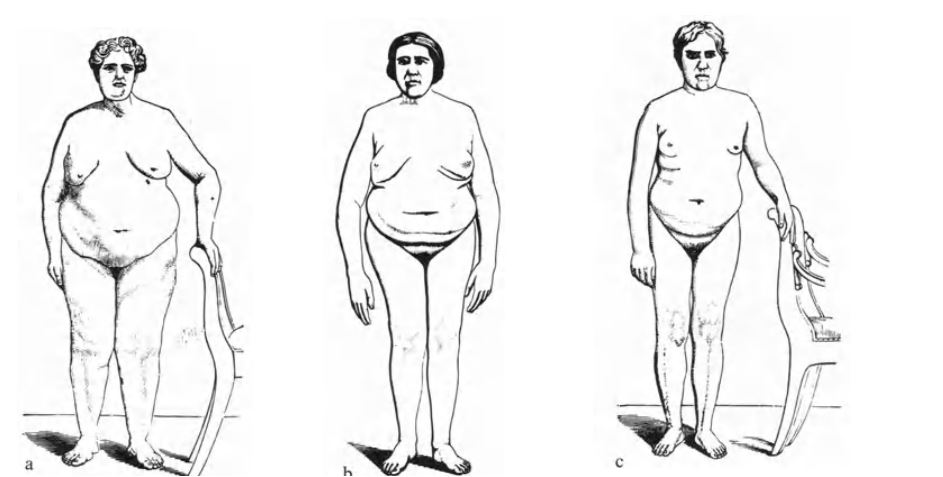
A: depicts a eunuch who developed hypogonadism very early on in life.
B: depicts the peripubertal onset of eunuchoidism, with a broad pelvis and narrow shoulders.
C: shows the postpubertal onset of eunuchoidism (maintains the narrow pelvis and broad shoulders of a normal male)
Features of Eunuchoidism
- Eunuchoid body habitus (meaning the arm span exceeds height). Eunuchoid proportions (upper/lower
body ratio <1 with an arm span >6 cm standing height) - Unbroken (high-pitched) voice with an absent Adam’s apple
- Poorly developed upper and lower extremity musculature
- Absent or poorly developed male pattern hair growth (mustache and beard)
- Infantile male genitalia. Prepubertal-sized
testes (1–3 mL) and microphallus (decrease in size of the penis but typically of normal length) - Cryptoorchidism
- Absence of baldness (remember that male pattern hair loss is testosterone-dependent)
What is the classic eunuchoid body shape or habitus?
This includes having relatively long arms and legs in relation to the trunk. Either the length of the lower part of the body (lower extremity) or 1/2 extended arm length (upper extremity) is typically greater than the length of the upper body.
Also, their average height lies a little above the normal height of corresponding population groups. However, it should be noted that these measurements can vary depending on the individual. In addition, patients with peripubertal onset of eunuchoidism tend to present with a narrow biacromial width (narrow shoulders) and a wide bitrochanteric diameter (broad pelvis).
A simple mnemonic for remembering the proportions of a eunuchoid habitus is that a eunuch is “a standing giant, but a sitting dwarf”. These eunuchoid body proportions are attributable to delayed fusion of the epiphyseal plate in the setting of testosterone deficiency.
What are the eunuchoid body proportions?
This is depicted in the line diagram below
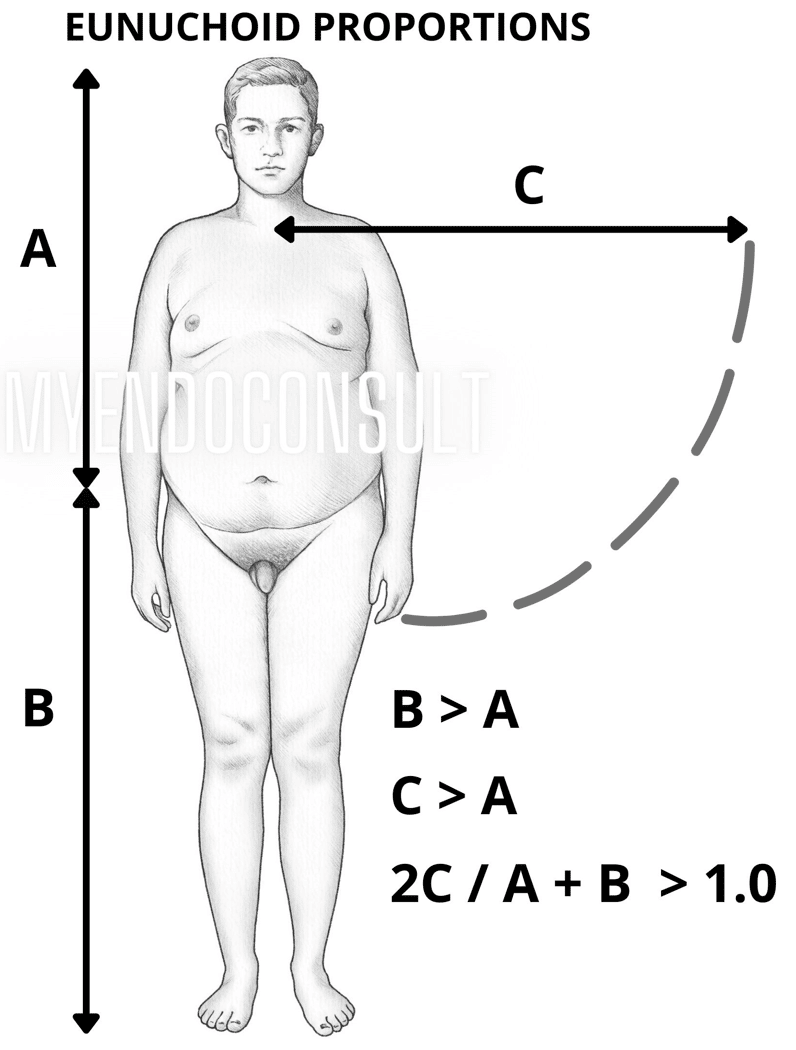
The ratio of upper body (A) to lower body (B) is less than 0.88. A/B <0.88
The ratio of a full arm span (C x 2 ) to full body height (A+B) is greater than 1.0. Formula = 2C/A+B >1.0
- A = Distance from the vertex to the symphysis pubis (upper body)
- B = Distance from the symphysis pubis to the heel (lower body)
- C = Distance from the sternum to the hand (50% arm span)
- Also, note the narrow shoulders and broad pelvis of this eunuch.
Eunuch Body Proportions (Simple Mnemonic)
Upper/Lower body ratio <1 with an arm span > 6 cm standing height
Causes of eunuchoidism
| Testicular failure | Pituitary failure |
| Klinefelter’s syndrome | Hypophysectomy (surgical or irradiation therapy) |
| Scrotal injury (torsion, hematoma, herniorrhaphy, unsuccessful orchidopexy) | Pituitary ischemia (cavernous sinus thromobosis) |
| Mumps orchitis | Hemochromatosis |
| Pelvic irradiation | Hypophysitis |
| Castration | Craniopharyngioma |
| Anorchia | Basal skull fracture (scarring of the hypophysis) |
First case report of Klinefelter Syndrome
Harry Klinefelter Jr worked with Dr. Fuller Albright (a luminary in the field of metabolic bone disease) during the 1940s as a “traveling fellow”. Dr. Albright tasked Dr. Klinefelter with the task of writing up a publication of 9 unique cases of men with gynecomastia, small testes, and additional features of Eunuchoidism.
The clinicopathologic features described in the case series submitted by Klinefelter, Albright, and Reifenstein to The Journal of Clinical Endocrinology represent the first attempt at elucidating the cause of Klinefelter Syndrome.
- Gynecomastia
- Azoospermia without the absence of Leydig cells (a-Leydigism)
- Increased serum follicle-stimulating hormone
- Testosterone-producing Leydig cells noted on testicular biopsy
- Elevated FSH due to the absence of a testicular hormone (now known as inhibin-B) other than testosterone. Inhibin B is produced by Sertoli cells in the seminiferous tubules.
Klinefelter Syndrome (A classic cause of Eunuchoidism)
Although Klinefelter et al were able to exclude testicular inflammation (or infection) or obstruction of the vas deferens, the underlying cause was unclear in 1942.
After the discovery of DNA, an additional X chromosome (or Barr Body) was identified in the tissue of subjects with Klinefelter Syndrome. In 1959, the association of an extra X chromosome with Klinefelter syndrome was confirmed.
It is currently clear that an extra X chromosome results in a dense mass of chromatin (also known as Barr body) within the nuclei of somatic cells. How this leads to testicular failure continues to remain unclear at this time.
References
Rochira V, Kara E, Carani C. The endocrine role of estrogens on human male skeleton. Int J Endocrinol. 2015;2015:165215.
Images(s) Courtesy
- Labhart, Alexis. Clinical endocrinology: theory and practice. Springer Science & Business Media, 2012.
- MyEndoconsult
Kindly Let Us Know If This Was helpful? Thank You!
Excellent Suggestion. Thank you!!!
I would add Kallmann to the list. Thanks for the article.