Management of CAH
Diagnosis of CAH
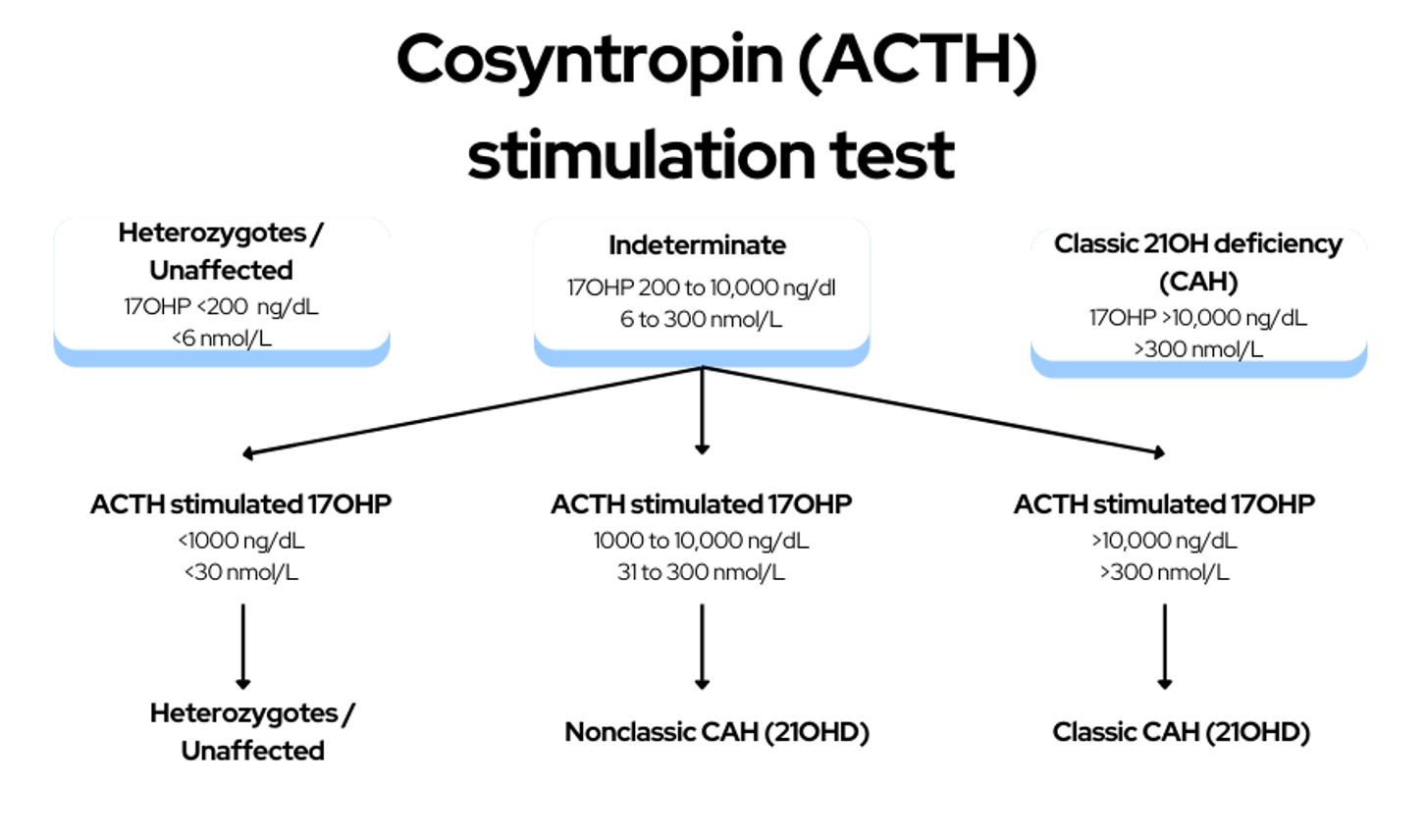
- Diagnosis of congenital adrenal hyperplasia (CAH) involves referral to pediatric endocrinologists and evaluation by cosyntropin stimulation testing in infants with positive newborn screens for CAH.
- Symptomatic individuals past infancy should undergo screening with an early-morning (before 8 AM) baseline serum 17-hydroxyprogesterone measurement by liquidchromatography–tandem mass spectrometry.
- Borderline 17-hydroxyprogesterone levels should prompt obtaining a complete adrenocortical profile after a cosyntropin stimulation test to differentiate 21-hydroxylase deficiency from other enzyme defects.
- Genotyping is suggested only when results of the adrenocortical profile after a cosyntropin stimulation test are equivocal, or cosyntropin stimulation cannot be accurately performed, or for purposes of genetic counseling. Genotyping at least one parent aids in the interpretation of genetic test results because of the complexity of the CYP21A2 locus.
Treatment of CAH
Treatment of classic congenital adrenal hyperplasia:
- Growing individuals with classic congenital adrenal hyperplasia should be given maintenance therapy with hydrocortisone.
- Oral hydrocortisone suspension and chronic use of long-acting potent glucocorticoids should be avoided in individuals with congenital adrenal hyperplasia.
- Fludrocortisone and sodium chloride supplements should be added to the treatment regimen in the newborn and early infancy.
- Adults with classic congenital adrenal hyperplasia should be given daily hydrocortisone and/or long-acting glucocorticoids plus mineralocorticoids, as clinically indicated.
- Monitoring for signs of glucocorticoid excess and inadequate androgen normalization is necessary to optimize the adrenal steroid treatment profile.
- Monitoring for signs of mineralocorticoid deficiency or excess is recommended in all individuals with classic congenital adrenal hyperplasia.
Need for stress dosing of steroids
Congenital adrenal hyperplasia (CAH) patients require glucocorticoid treatment for their entire lives. In case of certain situations, such as febrile illness, dehydration caused by gastroenteritis, major surgeries with general anesthesia, or major trauma, stress dosing is recommended. This means that patients should increase their glucocorticoid dosage to prevent adrenal crisis. However, in case of everyday mental and emotional stress, minor illness, and routine physical exercise, increased glucocorticoid doses are not necessary.
It is recommended that all patients with CAH should always wear or carry medical identification indicating that they have adrenal insufficiency. Moreover, patients, their guardians, and close contacts should be educated on the prevention of adrenal crisis and how to increase the dose of glucocorticoid (but not mineralocorticoid) during intercurrent illness. In addition, every CAH patient should be equipped with a glucocorticoid injection kit for emergency use and be educated on parenteral self-administration (young adult and older) or lay administration (parent or guardian) of emergency glucocorticoids.
Monitoring Guidelines
Regular monitoring is essential to ensure that the Treatment is effective and safe. The following are the recommended guidelines for monitoring therapy in patients with CAH
- Close monitoring is essential for infants ≤18 months of age, with evaluations recommended every three months in the first three months of life, followed by every four months after 18 months.
- Pediatric patients with CAH require regular assessments of growth velocity, weight, blood pressure, physical examinations, and biochemical measurements to evaluate the adequacy of glucocorticoid and mineralocorticoid replacement.
- Annual bone age assessments are recommended until near-adult height is attained for pediatric patients under the age of 2 years.
- Annual physical examinations, including assessments of blood pressure, body mass index, and Cushingoid features, and biochemical measurements to assess the adequacy of glucocorticoid and mineralocorticoid replacement, are recommended for adults with CAH.
- Consistently timed hormone measurements relative to medication schedule and time of day are recommended for monitoring Treatment in adults with CAH.
- Clinicians should avoid completely suppressing endogenous adrenal steroid secretion in adults with CAH to prevent adverse effects of overtreatment.
How about patients with NCCAH
Non-classic congenital adrenal hyperplasia (NCAH) is a milder form of congenital adrenal hyperplasia (CAH) that results from a partial deficiency in the enzyme 21-hydroxylase, which is responsible for producing cortisol and aldosterone. Unlike classic CAH, which is typically diagnosed in infancy, NCAH often presents in adolescence or adulthood and is often not diagnosed until later in life. NCAH can cause symptoms such as early onset of puberty, irregular menstrual cycles, excessive hair growth, and acne. It can also lead to fertility problems in women and decreased fertility in men. Treatment of NCAH involves managing symptoms with glucocorticoid therapy and regular monitoring to assess the effectiveness of Treatment.
These guidelines suggest the following for the management of nonclassic congenital adrenal hyperplasia:
- Glucocorticoid treatment is suggested for children and adolescents with early onset and rapid progression of pubarche or bone age and adolescent patients with overt virilization.
- Glucocorticoid treatment is not recommended for asymptomatic nonpregnant individuals with nonclassic congenital adrenal hyperplasia.
- The option of discontinuing therapy is suggested for previously treated patients with nonclassic congenital adrenal hyperplasia when adult height is attained or other symptoms resolve.
- Glucocorticoid treatment is suggested for adult women with nonclassic congenital adrenal hyperplasia who also have patient-important hyperandrogenism or infertility.
- Daily glucocorticoid therapy is generally not suggested for most adult males with nonclassic congenital adrenal hyperplasia, except for cases of infertility, testicular adrenal rest tumors or adrenal tumors, and phenotypes that are intermediate between classic and nonclassic phenotypes.
- Hydrocortisone stress dosing is suggested for major surgery, trauma, or childbirth in patients with nonclassic congenital adrenal hyperplasia only if they have a suboptimal cortisol response to cosyntropin or iatrogenic adrenal suppression.