Horner’s syndrome classically presents with anhidrosis, ptosis, miosis, and enophthalmos. The simple mnemonic, SAMPLE can be used to recall both the causes and clinical features of the syndrome.
Clinical features
A memory device for recalling the features of Horner syndrome is SAMPLE.
- Sympathetic Nerve Paresis
- Anhidrosis, Anisocoria (Difference in pupillary size)
- Miosis (Pupillary constriction)
- Ptosis
- Loss of the ciliospinal reflex
- Enophthalmos
Etiology
A simple Horner syndrome mnemonic is SAMPLE.
- Syringomyelia, Spinal trauma above the T2 spinal level, Spinal cord tumors and Stroke
- Arnold-Chiari malformation
- Meningitis, Multiple sclerosis
- Pituitary tumors
- Lateral medullary syndrome
- Encephalitis, Enlarged cervical masses
How does thyromegaly cause Horner Syndrome?
The superior cervical ganglion (SCG) serves as a relay center for higher-order neurons and has projecting from it, postganglionic neurons, which will eventually terminate in the orbit, skin of the head and neck region. The SCG lies near the thyroid and is subject to extrinsic compression in the setting of significant thyromegaly.
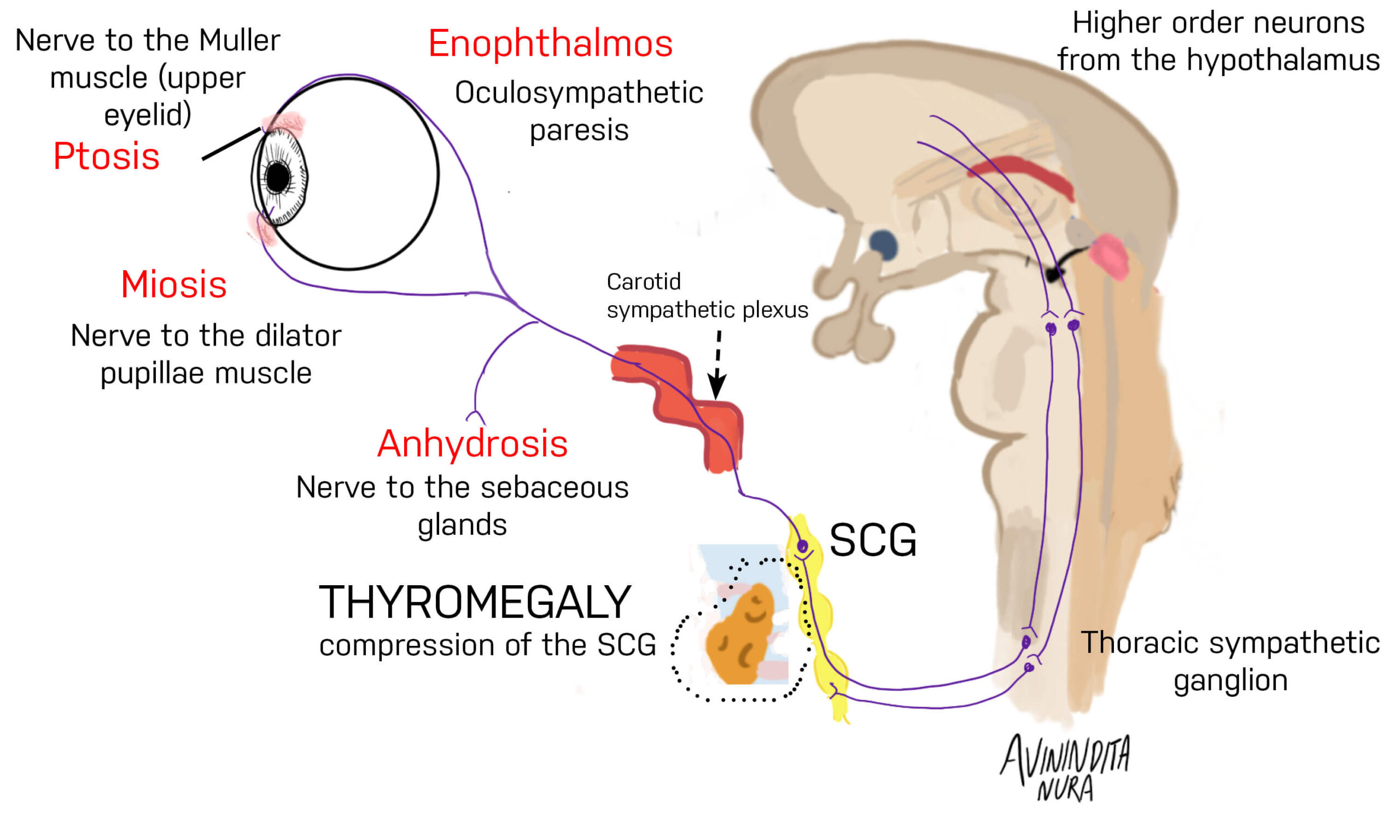
- Distal innervation of Muller’s muscle, dilator pupillae muscle, and sebaceous glands in the skin can be impaired by clinically significant thyromegaly (due to compression of the SCG).
- Motor neurons supplying Mullers muscle are involved, accounting for ptosis.
- The involvement of sympathetic innervation of the dilator pupillae muscle accounts for miosis.
- Loss of the ciliospinal relfex (pupillary dilation on compression of the neck)
- Enophthalmos occurs because of oculosympathetic paresis.
- Anhidrosis (an inability to sweat) occurs as a result of oculosympathetic paresis.
References
Kanagalingam S, Miller NR. Horner syndrome: clinical perspectives. Eye Brain. 2015;7:35-46. Published 2015 Apr 10.
Thompson HS. Johann Friedrich Horner (1831-1886). Am J Ophthalmol. 1986 Dec 15;102(6):792-5.
Images(s) Courtesy
MyEndoConsult