
The GKI or GIK regimen is a simple and effective combined insulin delivery method that has gained wide acceptance in the perioperative management of diabetic patients who would require Nil Per Oral (NPO) status. The GKI regimen can be used in patients with either type 1 or type 2 diabetes mellitus in the perioperative period.
It involves the continuous intravenous administration of insulin, glucose, and potassium as a single infusion. GKI is typically initiated on the morning of the surgery and continued until the patient resumes regular oral feeding.
Origin of the GKI regimen
The GIK or GKI regimen is based on the classic Alberti regimen, a treatment protocol for managing diabetes that involves administering glucose, insulin, and potassium. This approach was developed by Thomas and Alberti in the 1980s and has been proven effective in controlling blood sugar levels in patients with diabetes.
The GKI infusion regimen is based on the following metabolic principles
- A 70kg adult requires approximately 180 grams of glucose per day for both nervous system and red cell function (About 7.5 grams of glucose per hour)
- Insulin drives serum potassium into cells, increasing the risk for hypokalemia
- An insulin sensitivity factor of 1 unit for every 25mg/dl of capillary glucose
Remembering the components of the GKI infusion bag
A simple mnemonic or memory aid is the rule of 10s. 10% Dextrose, 10units of regular insulin, and 10mEq KCl
GKI protocol (The Classic Alberti Regimen)
The Alberti Regimen (1979) combines regular insulin, dextrose, and potassium in a single infusion. This helps to prevent inadvertent insulin infusion without dextrose, thus reducing the risk of hypoglycemia.
The amount of insulin added to a bag is dependent on the patient’s capillary glucose. For this reason, new mixtures of regular insulin with potassium and dextrose should be prepared when a dose change in insulin is needed.
Caution : It is worth noting that aspart, lispro, glulisine insulin CANNOT be administered intravenously. These insulins are only appropriate for subcutaneous administration.
On the morning of surgery, set up 500ml of 10% dextrose, 10 units of regular insulin, and 10 mmol of potassium chloride (Kcl). The recommended initial infusion rate is 100 ml per hour. Blood glucose should be checked every 1-2hours perioperatively. Capillary glucose guides subsequent changes in the GKI bag. Thus, the rate of infusion remains constant; however, the dose of regular insulin varies based on capillary glucose. See the infographic section below.
Before Surgery
- Do not administer any insulin secretagogues on the morning of surgery
- Discontinue metformin before surgery
- Set up an infusion of 500ml of 10% Dextrose, 10units of regular insulin, and 10mEq of potassium chloride (KCl). We will refer to this as the standard GKI. GKI should be initiated at least 30 minutes prior to surgery.
During surgery
- Start the infusion rate at 100ml per hour and monitor capillary glucose hourly throughout the surgery in order to maintain glycemic control. The subsequent infusion rate will be dependent on capillary blood glucose (checked at least every hour).
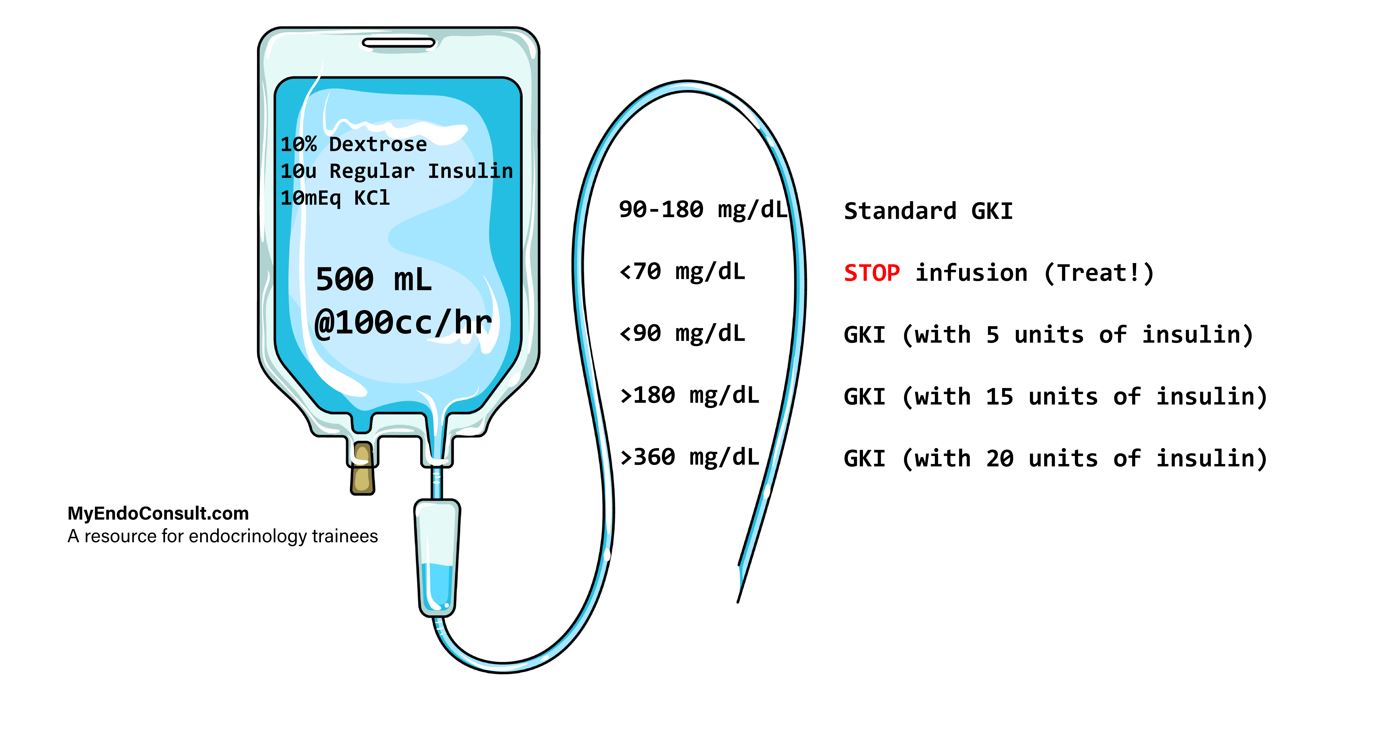
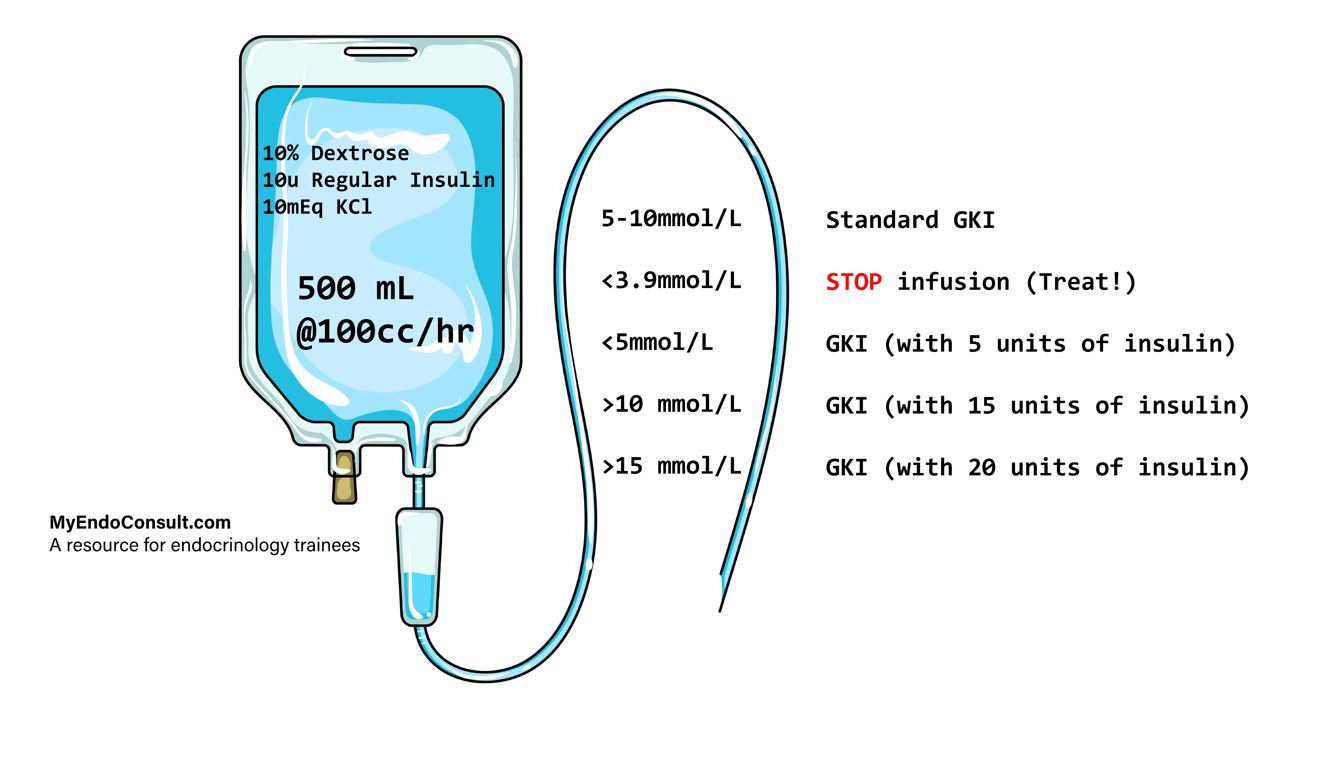
| Capillary glucose mmol/L (mg/dL) | Regimen |
| 5-10 mmol/L (90-180mg/dL) | Continue Standard GKI at 100ml per hour |
| <3.9 mmol/L (70mg/dL) | STOP infusion. Administer IV bolus of 50% Dextrose in water (25ml) |
| <5 mmol/L (90mg/dL) | Change bag to 500 ml of 10% Dextrose, 10mEq of KCl + 5 units of regular insulin, @100ml per hour |
| >10 mmol/L (180mg/dL) | Change bag to 500 ml of 10% Dextrose, 10mEq of KCl + 15 units of regular insulin, @ 100ml per hour |
| >20 mmol/L (360mg/dL) | Change bag to 500 ml of 10% Dextrose, 10mEq of KCl + 20 units of regular insulin, @ 100ml per hour |
After surgery
- Continue 4-5 hourly infusions of the glucose potassium insulin bag (500ml at 100cc per hour) and monitor capillary blood glucose every 4 hours and plasma potassium every 8 hours. If smaller volumes of fluids have to be administered due to a change in the patient’s clinical status, then equivalently lower volumes of either 20% or 50% Dextrose may be used (via a central line due to the higher concentration and risk for phlebitis!)
- Stop the GKI infusion when oral feeding is resumed and switch to multiple daily insulin injections. Do NOT use a reactive sliding scale only for a diabetic patient who has resumed oral feeding.
- If oral feeding cannot be resumed within 48-72hours, as might occur with critically ill patients, consider parenteral nutrition.
The Modified Alberti Regimen
The modified Alberti Regimen is much simpler since the optimal glucose range is much broader (120-200mg) and requires no change in the bag when capillary glucose is in this range. This will mean less frequent changes in GKI bags.
On the morning of surgery, set up 500ml of 10% dextrose, 15 units of regular insulin (slighter higher dose than the classic Alberti regimen), and 10 mmol of potassium chloride (Kcl).
The recommended initial infusion rate is 100 ml per hour. Blood glucose should be checked every 1-2hours perioperatively.
| Capillary glucose mmol/L (mg/dL) | Regimen |
|---|---|
| 6.7 – 11.1 mmol/L (120-200 mg/dL) | Continue Modified Alberti (GKI bag - 500ml of 10% Dextrose, 15units of Regular Insulin and 10mEq of potassium chloride) at 100ml per hour |
| < 6.7 mmol/L (120mg/dL) | Change bag to 500 ml of 10% Dextrose, 10mEq of KCl + 10 units of regular insulin, @100ml per hour |
| > 11.1 mmol/L (200mg/dL) | Change bag to 500 ml of 10% Dextrose, 10mEq of KCl + 20 units of regular insulin, @100ml per hour |
Caveats to applying the GKI regimen
- Patients who are septic or undergoing cardiac bypass surgery typically have higher insulin requirements in the perioperative period.
- If the infusion is stopped for more than 30 minutes, the patient’s extracellular fluid will have inadequate exogenous insulin; thus, close monitoring is required. This is even more relevant for patients with type 1 diabetes mellitus. Without any background basal insulin, these patients can go into rapid diabetic ketoacidosis!
- As with all things in medicine, specifically diabetes care, every patient is unique. Therefore, common sense and clinical judgment are required when starting the standard GKI regimen.
Simple Infographics for the Classic Alberti GKI regimen
The infographics below depict suggested infusion rates depending on blood glucose levels. Scales of measurement in either mg/dl or mmol/L.
- What is the rule of 10s for the GKI (Alberti) infusion?
This refers to a bag of 500ml of 10% Dextrose, 10units of regular insulin, and 10mEq of potassium chloride (KCl).
- When should the GKI infusion be started?
GKI should be initiated at least 30 minutes prior to surgery.
- When should the GKI infusion be stopped?
Stop the GKI infusion when oral feeding is resumed and switch to multiple daily insulin injections.
References
- Alberti KG, Thomas DJ. The management of diabetes during surgery. Br J Anaesth. 1979 Jul;51(7):693-710.
- Thomas DJ, Platt HS, Alberti KG. Insulin-dependent diabetes during the perioperative period. An assessment of continuous glucose-insulin-potassium infusion, and traditional treatment. Anaesthesia. 1984 Jul;39(7):629-37.
Images(s) Courtesy
MyEndoConsult