Renee Descartes described the pineal gland as the “seat of the soul.” It is located in the center of the brain. The primary function of the pineal gland is to receive signals about the state of the light-dark cycle from the immediate environment and then transmit this information by producing and secreting melatonin. Melatonin is produced and secreted in a rhythmic pattern.
Melatonin is mostly secreted during the dark period of the day, and serves extensively as the marker of the circadian clock.
Melatonin is also used as a therapy for some sleep disorders such as jet lag, non-24h sleep-wake disorders, and delayed sleep phase syndrome.
Melatonin might have more therapeutic uses in the future, considering that many physiological roles have been attributed to melatonin. The physiological effects of melatonin are exerted during night or night. It is also effective when suitably administered during the daytime when melatonin levels are at their lowest. Melatonin is also involved in neuroprotection, cell protection, the reproductive system, and other functions. The physiological function of the pineal gland may be impaired by developmental and accidental conditions, including craniopharyngiomas, pineal tumors, injuries that affect the pineal sympathetic innervation, as well as congenital disorders that affect the secretion of melatonin. This article highlights the anatomy and physiology of the pineal gland.
Anatomy & physiology of the pineal gland
Location and structure
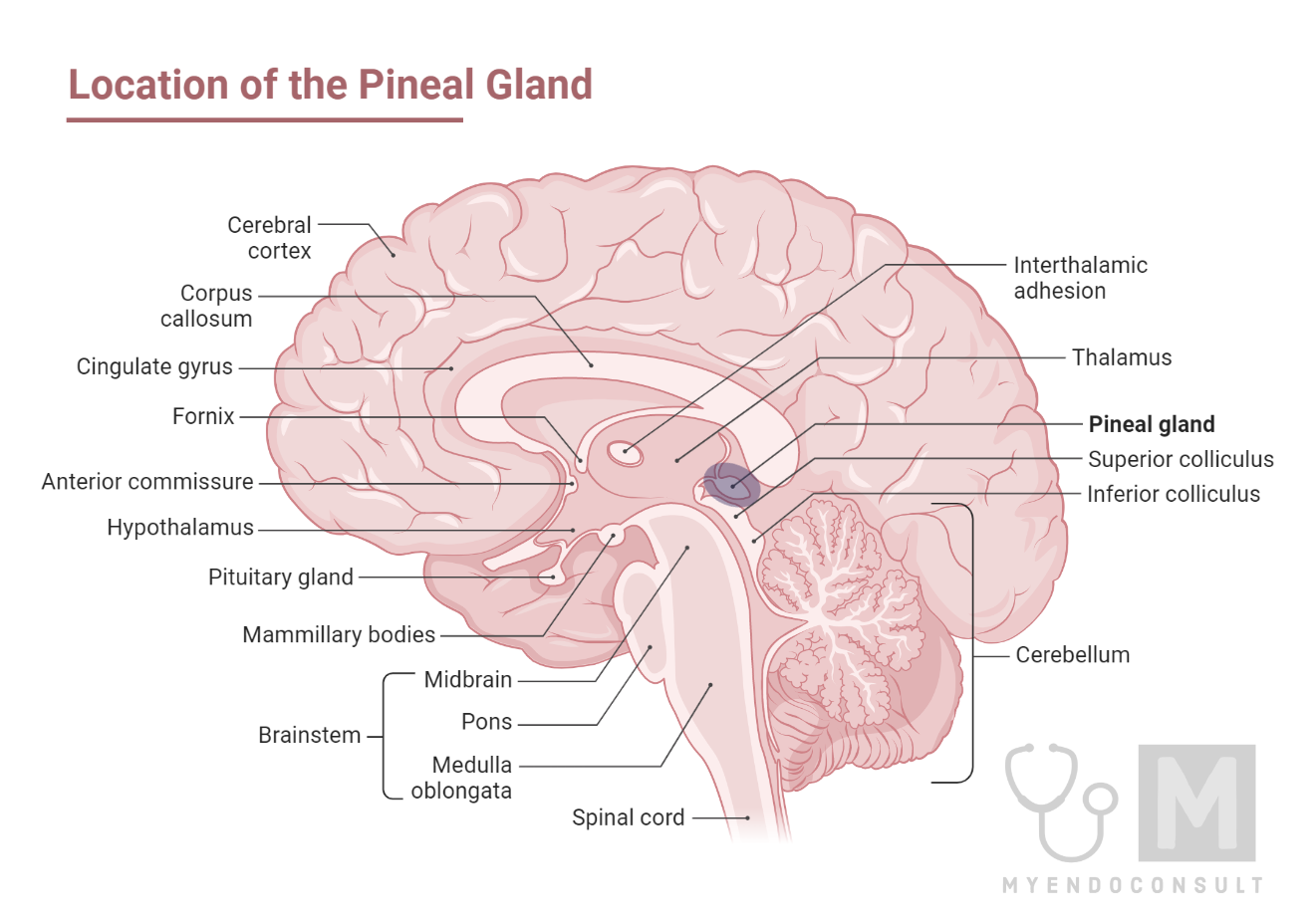
The pineal gland is a neuroendocrine structure comprising a part of the epithalamus (a division of the diencephalon). The epithalamus’s other components are the habenular nuclei, stria medullaris, paraventricular nuclei, and posterior commissure.
The pineal gland starts as an outward projection from the posterior wall of the third ventricle, just below the splenium of the corpus callosum. It is located in the groove between the superior colliculi and has a bilateral link to the posterior aspects of both thalami.
Innervation and blood supply
The human pineal gland calcifies with age providing an excellent imaging marker.1 The pineal gland is innervated by the sympathetic nervous system. The sympathetic innervation of the pineal gland arises from the superior cervical ganglia.2 Both the anterior and posterior circulation supplies the arterial vascularization of the pineal gland, being the primary artery supplying the lateral pineal artery, which starts out from the posterior circulation. 3
Cell types
The primary cell types in mammals are the pinealocytes which make up 95% of the cells in the pineal gland, follosed by the phagocytic and astrocytic cells (all glial cells).4 Pinealocytes are involved in melatonin synthesis and secretion.
The pineal stalk connects the pineal gland to the rest of the brain. The pineal stalk divides into the inferior and the superior laminae. The inferior laminae contain the posterior commissure while the superior laminae contain the habenular commissure. The pineal recess of the third ventricle fills the space between the laminae. The pineal gland parenchyma consists mostly of clusters and cords of pinealocytes and neuroglial cells. The neuroglial cells are the main component of the pineal stalk.
The pineal gland also contains the brain sand or corpora arenacea. Corpora arenacea are calcium, phosphate and carbonate deposits that form multilaminar corpuscles. These deposits accumulate with age and are byproducts of secretory activity. The corpora arenacea is significant in clinical situations because they serve as landmarks in radiologic tests. They are also used in microscopic identification of the pineal gland.
Functions of the pineal gland
Regulation of circadian rhythms
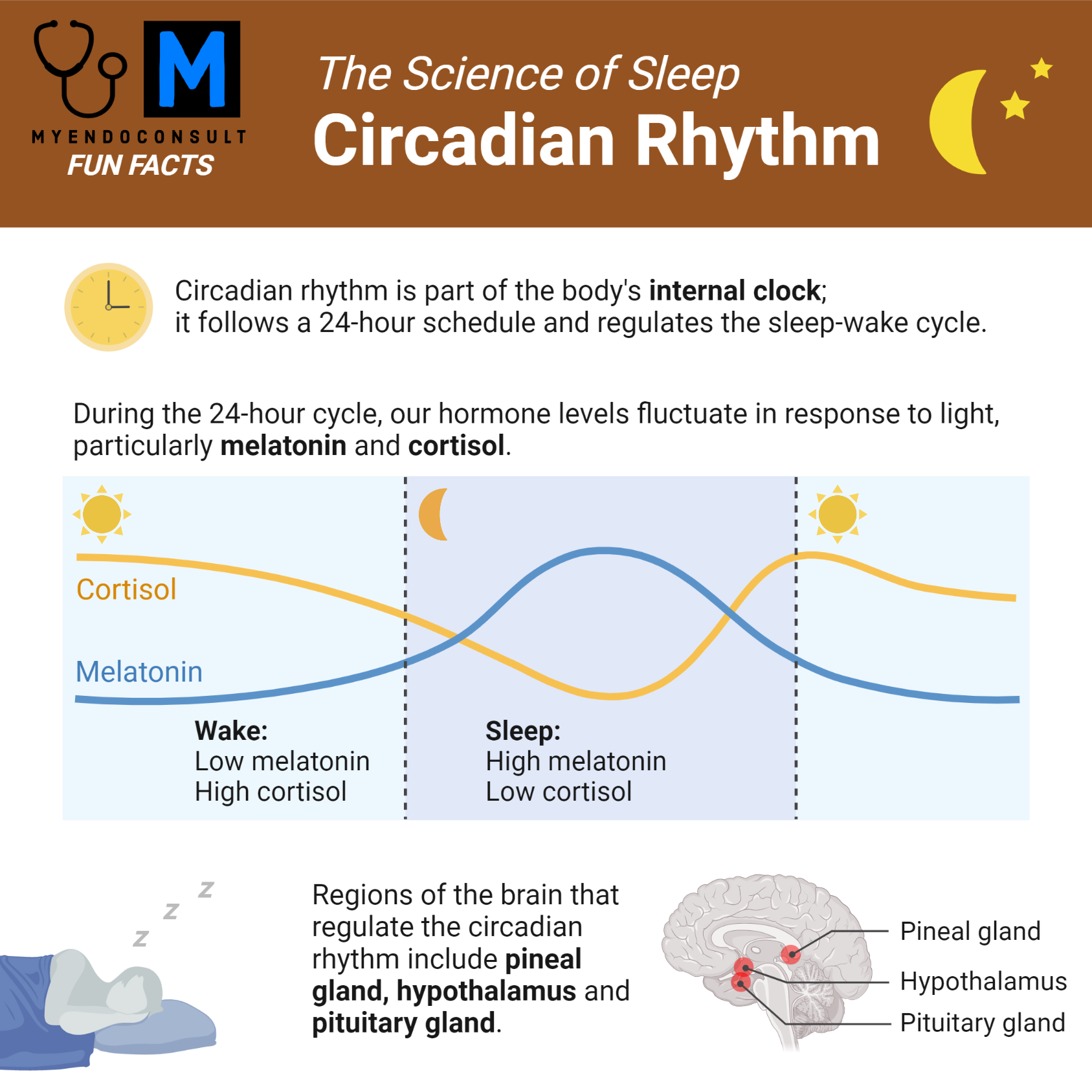
The circadian rhythm is an internal biological clock the regulates sleep-wake cycle, and undergoes a 24-hour repetitive occurrence. The circadian rhythm is regulated by the rising and falling of melatonin concentrations. It is basically an intrinsic mechanism that allows for the synchronization of the body’s physiological processes.
The signals from daylight and night rhythm are transmitted through the retinohypothalamic tract to the pineal gland. The transmissions of these signals occur by the following route:
- Light falls on the retina. An action potential is triggered in response and transmitted to the suprachiasmatic nucleus of the hypothalamus through the retinal fibers.
- This is followed by a relay of the information to the paraventricular nucleus of the hypothalamus. The paraventricular nucleus projects fibers to the intermediolateral nucleus in the lateral column of the spinal cord.
- The impulses are transmitted by the postganglionic fibers of the cervical sympathetic chain to the pineal gland.
The pineal gland receives signals about the light that hits the eyes through the hypothalamus. With these, the pineal gland can regulate the circadian rhythm via melatonin secretion. This unique connection to the eyes and the ability of the pineal gland to respond to light is the reason why it is referred to as the “third eye.”
Secretion of melatonin (Synthesis and release of melatonin)
The synthesis of melatonin (N-acetyl-5-methoxytryptamine) occurs within the pinealocytes from tryptophan. Melatonin synthesis occurs mostly during the dark, when there is an increase in serotonin-N-acetyltransferase activity – a factors responsible for 5-hydroxytryptamine conversion to N-acetylserotonin. N-acetylserotonin is then converted to melatonin by acetylserotonin O-methyltransferase. Studies have shown that there is usually a drastic decline in synthesis of serotonin with light treatment at night – a process which seems to depend on proteasomal proteolysis.5 Availability of serotonin and arylalkylamine N-acetyltransferase (AA-NAT) are involved in reducing melatonin production. There is high expression of AA-NAT in the retina, pineal gland, and in the pituitary, other parts of the brain, and the testis. Synthesis of melatonin is described in other sites. Activation of AA-NAT is stimulated by the activation of α1b adrenergic receptors and β1 receptors by norepinephrine. Norepinephrine is the primary neurotransmitter via β-1 adrenoreceptors potentiated by α-1 stimulation. Norepinephrine levels increases at night.
Physiological effects of melatonin on the body
Melatonin is designed to act at every level of the organism. As such, its actions are multiple and diversified with prospective or multiple effects. The prospective effects occur during the previous day, while immediate actions involving endogenous melatonin occur at night.
The role of melatonin in the regulation of core body temperature
Melatonin is involved in circadian thermoregulation. The peaking of melatonin is associated with a fall in body temperature, tiredness, and a fall in performance and mental alertness.6 This association is reproduced by exogenous administration of melatonin during the daytime, resulting in sleepiness and fatigue, and a fall in body temperature.6
Melatonin and glucose homeostasis/energy metabolism
Melatonin plays an important role in glucose homeostasis and energy metabolism (high insulin sensitivity, lipogenesis, glycogen synthesis, and a sleep phase where energy stored is utilized).7
In a randomized placebo-controlled trial published in the journal Clinical Endocrinology, researchers found that administration of melatonin in post-menopausal women resulted in a drastic reduction in fat mass followed by an increase in lean mass.8
Night-time secretion of melatonin enhances diurnal sensitivity and preserves the mass and function of beta cells.9 Studies have also shown that low secretion of melatonin is a major risk factor for type 2 diabetes (T2DM).10
Hyperglycemia and insulin resistant is a common occurrence in short sleepers. Both phenomena can also be observed when there is a misalignment between wake time and melatonin secretion. Administration of melatonin can lead to hyperglycemia and iatrogenic insulin resistance in the mornings, based on the time of administration as well as the subject’s metabolizing characteristics.
Recent studies have revealed that certain variants of the gene that encodes for MT-1B have been linked with suboptimal beta-cell function and an increased risk for type 2 diabetes mellitus.11 It is also worth mentioning that certain cardiovascular effects such as regulation of heart rate, vascular resistance, and antihypertensive properties have been attributed to melatonin.12, 13
Other functions of the pineal gland
Role of the pineal gland in the regulation of seasonal breeding
The control of sexual maturity by the neuroendocrine system is heavily influenced by the pattern in which melatonin is secreted. It is important to note that the timing of puberty is determined by melatonin secretion (through the photoperiod) in some species.14
Studies have shown that melatonin inhibits gonadotrophin-releasing hormone and consequently stops the release of luteinizing hormone, a clear indication that melatonin is involved in the timing of developmental phases.15 Kisspeptin is believed to mediate melatonin inhibition of GnRH secretion. Low levels of melatonin have been linked to precocious puberty while high levels of melatonin contribute to hypothalamic amenorrhea and delayed puberty.16, 17
There are inconsistent data on circulating levels of melatonin and its variation during the female menstrual cycle.18 High doses of melatonin in males (100 mg/day) potentiate LH suppression induced by testosterone. Studies have also reported a negative correlation between melatonin and nocturnal serum LH.19, 20
However, the many attempts to develop a contraceptive pill with melatonin and progestin have been unsuccessful.21 People who live in the artic region tend to experience lower rates of conception during the winter where melatonin levels are always high, compared to the summer. In summary, many human studies agree that melatonin is inhibitory to reproductive function.
Role of the pineal gland in immune function and aging
Many studies have attributed anti-aging and antioxidant properties to melatonin. Melatonin has an in vitro antioxidant and free radical scavenging property22-24 preventing oxidative damage in DNA, protein, and lipids. Melatonin reduces oxidative stress more efficiently than glutathione, owing to its high concentration in the mitochondria. Even though most of these effects have manifested in supraphysiological doses of melatonin, the exact dose of exogenous melatonin needed to generate significant antioxidant activity is yet to be established.
Clinical relevance of the pineal gland
Disorders of the pineal gland can impact the production of melatonin, resulting in disruptions to the body’s natural rhythms. These disorders can range from benign conditions, such as pineal gland cysts and calcifications, to more serious conditions, such as pineal gland tumors. Additionally, disorders that disrupt circadian rhythms, such as jet lag and shift work disorder, can also affect the pineal gland’s function.
Calcification
The pineal gland gets calcified easily. In fact, it gets calcified so much that it is used as a marker on x-rays. There is a direct correlation between calcium and phosphate deposits and age. It is important to note that there is an association between corpora arenacea and pineal gland calcification. Studies have shown that there is a higher degree of pineal calcification in Alzheimer patients compared to other types of dementia. It is also important to note that the correlation between pineal gland calcification and cluster/migraine headaches is loose.
Tumors
Several tumors may develop from the pineal gland. Making a correct diagnosis of the tumor is important for treatment. Hydrocephalus is usually the primary symptom of the tumor. Invasion of the thalamus by the pineal gland may cause loss of sensation and weakness in some part of the body. Pineal invasion of the hypothalamus may affect water and temperature regulation, trigger weight gain and disrupt sleep.
The size and location of the tumor can be seen with an MRI. The type of tumor can be determined with a biopsy. A biopsy is usually done through an endoscopic or stereotactic procedure. Biomarkers are sometimes used to detect whether or not a tumor is present. If the biomarker is found in the blood and cerebrospinal fluid, then a biopsy might not be required. Some of these biomarkers include carcinoembryonic antigen, beta-human chorionic gonadotropin, and a-fetoprotein.
Retinal degeneration
Retinal degeneration hinders light appreciation. In this case, the retina will be insensitive to changes in light. Low levels of light will stimulate melatonin secretion.25
Jet lag
The sleep-wake cycle is usually disturbed when one travels across multiple time zones. It will require several days to adjust melatonin to the day-night pattern.
Disorders of the circadian rhythm
The retino-hypothalamic pineal pathway is stimulated by light during the daytime. Cells of the retinal ganglion activates the suprachiasmatic nucleus via the optic nerve. Suprachiasmatic nucleus inhibits the superior cervical ganglion through a complex network, thus inhibiting the sympathetic nervous system and preventing the release of melatonin from the pituitary gland into the circulation. In the dark, the inactivation of the suprachiasmatic nucleus causes a stimulation of the sympathetic nervous system, resulting in the release of melatonin by the pineal gland.26, 27
The commonest disorders associated with disruption of the circadian rhythm include delayed sleep phase and advanced sleep phase syndrome.28 Melatonin plays an important role in delayed sleep phase syndrome and sleep onset insomnia.
Parinaud syndrome
Pinealoma (tumor of the pineal gland) causes Parinaud syndrome by compressing regions in the dorsal midbrain due to progressive gland enlargement. Pineal gland tumor is one of the commonest causes of Parinaud syndrome in young adults. Many patients may experience diplopia and progressive blurring of vision.30
Melatonin supplementation in the treatment of sleep disorders
Over 200 randomized clinical trials on melatonin use have been published. The therapeutic uses of melatonin include cancer, neuroprotection and sleep disorders. Melatonin has been recommended for delayed sleep phase syndrome, jet lag, and non-24-hour sleep wake disorder syndrome by the American Academy of Sleep Science.31
Researchers have synthesized several melatonin receptor agonists, with some agonists having a higher affinity for melatonin receptor than endogenous melatonin. For instance, Ramelteon, a selective MT1/MT2 agonist is marketed as treatment for sleep onset insomnia. Agomelatine acts on the serotonin-2C receptor as anti-depressant, while tasimelton, an MT1/MT2 agonist is marketed for the treatment of circadian rhythm disorders especially non-24-hour sleep-wake disorder.32, 33
No consensus has been reached regarding melatonin dosage. There are varying dose formulations, and the usage depends on the clinical application. Patients are generally advised to begin with the lowest dose possible. Doses within the range of 0.1 – 0.3 mg/day may be administered for central clock synchronization. Such low produce melatonin at physiological concentrations. Doses ranging from 0.6 – 5 mg/day are used for sleep disorders, while doses exceeding 300 mg/day are used for the treatment of neurodegenerative disorders.34, 35
Conclusion
Based on the review of anatomical and physiological aspects of the pineal gland, we may conclude that:
- The pineal gland is sensitive to light and has a multi-neuronal phototransduction path
- Downregulation and upregulation of pineal hormones occur in the light and dark respectively.
- The pineal gland is thermoregulatory. It regulates the sex pattern and the sleep-wake cycle.
- Nearly all studies agree that the pineal gland is a photo-neuroendocrine organ that forms an integral part of the brain.
- The pineal gland offers information on seasonal and circadian rhythms, and connects the outside world with the biochemical and physiological needs of the internal systems.
- The role of the pineal gland is embedded in endocrinological, neurological, and psychiatric conditions due to the secretory actions of melatonin, serotonin, and N, N-dimethyl-tryptamine.
There is need for further research into the secretions of the pineal gland and how they interact with state of consciousness so as to have a better understanding of their physiological and clinical significance. Having a proper understanding of these molecules will facilitate the screening of parenchymal tumors in instances of atypical behavioral changes. It is also necessary to quantify the effect of melatonin on immunity, antioxidation, neuroplasticity, and homeostasis.
References
- Tan DX, Xu B, Zhou X, Reiter RJ. Pineal Calcification, Melatonin Production, Aging, Associated Health Consequences and Rejuvenation of the Pineal Gland. 2018;23(2)
- Kappers JA. Innervation of the Vertebrate Pineal Organ. In: Axelrod J, Fraschini, F., Velo, G.P. (eds) editor1983.
- Kahilogullari G, Ugur HC, Comert A, Brohi RA, Ozgural O, Ozdemir M, et al. Arterial vascularization of the pineal gland. Childs Nerv Syst. 2013;29(10):1835–41
- Moller M, Baeres FM. The anatomy and innervation of the mammalian pineal gland. Cell Tissue Res. 2002;309(1):139–50.
- Gastel JA, Roseboom PH, Rinaldi PA, Weller JL, Klein DC. Melatonin production: proteasomal proteolysis in serotonin N-acetyltransferase regulation. Science (New York, NY). 1998;279(5355):1358–60
- Cagnacci A, Elliott JA, Yen SS. Melatonin: a major regulator of the circadian rhythm of core temperature in humans. J Clin Endocrinol Metab. 1992;75(2):447–52.
- Picinato MC, Haber EP, Carpinelli AR, Cipolla-Neto J. Daily rhythm of glucose-induced insulin secretion by isolated islets from intact and pinealectomized rat. J Pineal Res. 2002;33(3):172–7.
- Amstrup AK, Sikjaer T, Pedersen SB, Heickendorff L, Mosekilde L, Rejnmark L. Reduced fat mass and increased lean mass in response to 1 year of melatonin treatment in postmenopausal women: A randomized placebo-controlled trial. Clin Endocrinol (Oxf). 2016;84(3):342–7.
- Costes S, Boss M, Thomas AP, Matveyenko AV. Activation of Melatonin Signaling Promotes beta-Cell Survival and Function. Mol Endocrinol. 2015;29(5):682–92.
- McMullan CJ, Schernhammer ES, Rimm EB, Hu FB, Forman JP. Melatonin secretion and the incidence of type 2 diabetes. 2013;309(13):1388–96.
- Prokopenko I, Langenberg C, Florez JC, Saxena R, Soranzo N, Thorleifsson G, et al. Variants in MTNR1B influence fasting glucose levels. Nat Genet. 2009;41(1):77–81
- Scheer FA, Van Montfrans GA, van Someren EJ, Mairuhu G, Buijs RM. Daily nighttime melatonin reduces blood pressure in male patients with essential hypertension. 2004;43(2):192–7
- Grossman E, Laudon M, Yalcin R, Zengil H, Peleg E, Sharabi Y, et al. Melatonin reduces night blood pressure in patients with nocturnal hypertension. Am J Med. 2006;119(10):898–902.
- Ebling FJ, Foster DL. Pineal melatonin rhythms and the timing of puberty in mammals. 1989;45(10):946–54
- Martin JE, Sattler C. Selectivity of melatonin pituitary inhibition for luteinizing hormone-releasing hormone. 1982;34(2):112–6
- Waldhauser F, Boepple PA, Schemper M, Mansfield MJ, Crowley WF Jr. Serum melatonin in central precocious puberty is lower than in age-matched prepubertal children. J Clin Endocrinol Metab. 1991;73(4):793–6.
- Berga SL, Mortola JF, Yen SS. Amplification of nocturnal melatonin secretion in women with functional hypothalamic amenorrhea. J Clin Endocrinol Metab. 1988;66(1):242–4.
- Parry BL, Berga SL, Mostofi N, Klauber MR, Resnick A. Plasma melatonin circadian rhythms during the menstrual cycle and after light therapy in premenstrual dysphoric disorder and normal control subjects. J Biol Rhythms. 1997;12(1):47–64
- Anderson RA, Lincoln GA, Wu FC. Melatonin potentiates testosterone-induced suppression of luteinizing hormone secretion in normal men. Hum Reprod. 1993;8(11):1819–22.
- Luboshitzky R, Wagner O, Lavi S, Herer P, Lavie P. Abnormal melatonin secretion in hypogonadal men: the effect of testosterone treatment. Clin Endocrinol (Oxf). 1997;47(4):463–9
- Voordouw BC, Euser R, Verdonk RE, Alberda BT, de Jong FH, Drogendijk AC, et al. Melatonin and melatonin-progestin combinations alter pituitary-ovarian function in women and can inhibit ovulation. J Clin Endocrinol Metab. 1992;74(1):108–17
- Karasek M. Melatonin, human aging, and age-related diseases. Exp Gerontol. 2004;39(11-12):1723–9.
- Reiter RJ, Mayo JC, Tan DX, Sainz RM, Alatorre-Jimenez M, Qin L. Melatonin as an antioxidant: under promises but over delivers. J Pineal Res. 2016;61(3):253–78
- Tan DX, Reiter RJ, Manchester LC, Yan MT, El-Sawi M, Sainz RM, et al. Chemical and physical properties and potential mechanisms: melatonin as a broad spectrum antioxidant and free radical scavenger. Curr Top Med Chem. 2002;2(2):181–97
- Meneses-Santos D, Buonfiglio DDC, Peliciari-Garcia RA, Ramos-Lobo AM, Souza DDN, Carpinelli AR, Carvalho CRO, Sertie RAL, Andreotti S, Lima FB, Afeche SC, Fioretto ET, Cipolla-Neto J, Marçal AC. Chronic treatment with dexamethasone alters clock gene expression and melatonin synthesis in rat pineal gland at night. Nat Sci Sleep. 2018;10:203-215
- Bass J, Takahashi JS. Circadian rhythms: Redox redux. 2011 Jan 27;469(7331):476-8.
- Reddy S, Reddy V, Sharma S. StatPearls [Internet].StatPearls Publishing; Treasure Island (FL): May 8, 2022. Physiology, Circadian Rhythm.
- Khan S, Nabi G, Yao L, Siddique R, Sajjad W, Kumar S, Duan P, Hou H. Health risks associated with genetic alterations in internal clock system by external factors. Int J Biol Sci. 2018;14(7):791-798.
- Bruni O, Alonso-Alconada D, Besag F, Biran V, Braam W, Cortese S, Moavero R, Parisi P, Smits M, Van der Heijden K, Curatolo P. Current role of melatonin in pediatric neurology: clinical recommendations. Eur J Paediatr Neurol. 2015 Mar;19(2):122-33
- Feroze KB, Patel BC. StatPearls [Internet].StatPearls Publishing; Treasure Island (FL): Aug 1, 2022. Parinaud Syndrome
- Morgenthaler TI, Lee-Chiong T, Alessi C, Friedman L, Aurora RN, Boehlecke B, et al. Practice parameters for the clinical evaluation and treatment of circadian rhythm sleep disorders. An American Academy of Sleep Medicine report. 2007;30(11):1445–59.
- Loiseau F, Le Bihan C, Hamon M, Thiebot MH. Antidepressant-like effects of agomelatine, melatonin and the NK1 receptor antagonist GR205171 in impulsive-related behaviour in rats. Psychopharmacology (Berl). 2005;182(1):24–32
- Arendt J, Rajaratnam SM. Melatonin and its agonists: an update. Br J Psychiatry. 2008;193(4):267–9
- Weishaupt JH, Bartels C, Polking E, Dietrich J, Rohde G, Poeggeler B, et al. Reduced oxidative damage in ALS by high-dose enteral melatonin treatment. J Pineal Res. 2006;41(4):313–23
- Zhdanova IV, Wurtman RJ, Morabito C, Piotrovska VR, Lynch HJ. Effects of low oral doses of melatonin, given 2-4 hours before habitual bedtime, on sleep in normal young humans. 1996;19(5):423–31