The secretin stimulation test is used in the timely diagnosis of gastrinoma in Zollinger Ellison Syndrome/multiple endocrine neoplasia type I syndrome. A positive secretin stimulation test allows the expedited diagnosis of gastrinomas and is helpful in patients with borderline or even normal levels of nonstimulated fasting serum gastrin.

What is secretin?
Secretin (discovered by Starling) is a 27 amino acid peptide produced by various tissues in the human body, including the small intestine, hypothalamus, and neocortex. Secretin binds to its cognate receptors present on pancreatic ductal and acinar cells and mediates the secretion of a bicarbonate-rich fluid that is critical in neutralizing gastric acid present in the small intestine.
Rationale of the Secretin Stimulation test
secretin stimulates the release of pancreatic juices while inhibiting gastric acid secretion and intestinal motility at the same time. In normal physiology, secretin stimulates the release of pancreatic fluid (containing bicarbonate), which, upon reaching the duodenal plays a pivotal role in neutralizing gastric acid and raising the duodenal pH. In so doing, this exerts a negative feedback inhibition which regulates the release of secretin.In patients with gastrin secreting tumors, secretin causes a paradoxical increase in the release of gastrin instead of its inhibition, as occurs in normal physiology. This forms the basis of the secretin stimulation test performed to diagnose hypergastrinemia.
Testing conditions
Antacids and proton pump inhibitors suppress gastric acid secretion and may alter the test results; consequently, they should be stopped at least 72 hours or two weeks before the secretin stimulation tests, respectively1.For patients with elevated basal gastrin levels, it is reasonable to rule out concomitant chronic atrophic gastritis or Helicobacter pylori infection before the test.
Secretin Stimulation Test procedure
- The patient should have fasted for at least 12 hours before the test.
- An intravenous cannula (heplock) should be placed for easy venous access throughout the test
- A venous blood sample is drawn at baseline to determine basal fasting serum gastrin levels before the secretin injection. At least two baseline gastrin levels should be drawn.
- An intravenous bolus of secretin is injected over 30 seconds (0.4mcg per kg body weight of synthetic human secretin).
- Post secretin gastrin levels will then be obtained at 2, 5, 10, 15, and 20 minutes (gold top tube).
- Discontinued intravenous access and label samples appropriately.
Various diagnostic thresholds have been proposed by different authors with varying sensitivities and specificities. A rise in gastrin levels after secretin administration (compared to baseline) of ≥200 pg/mL, ≥120 pg/mL, or 110 pg/mL.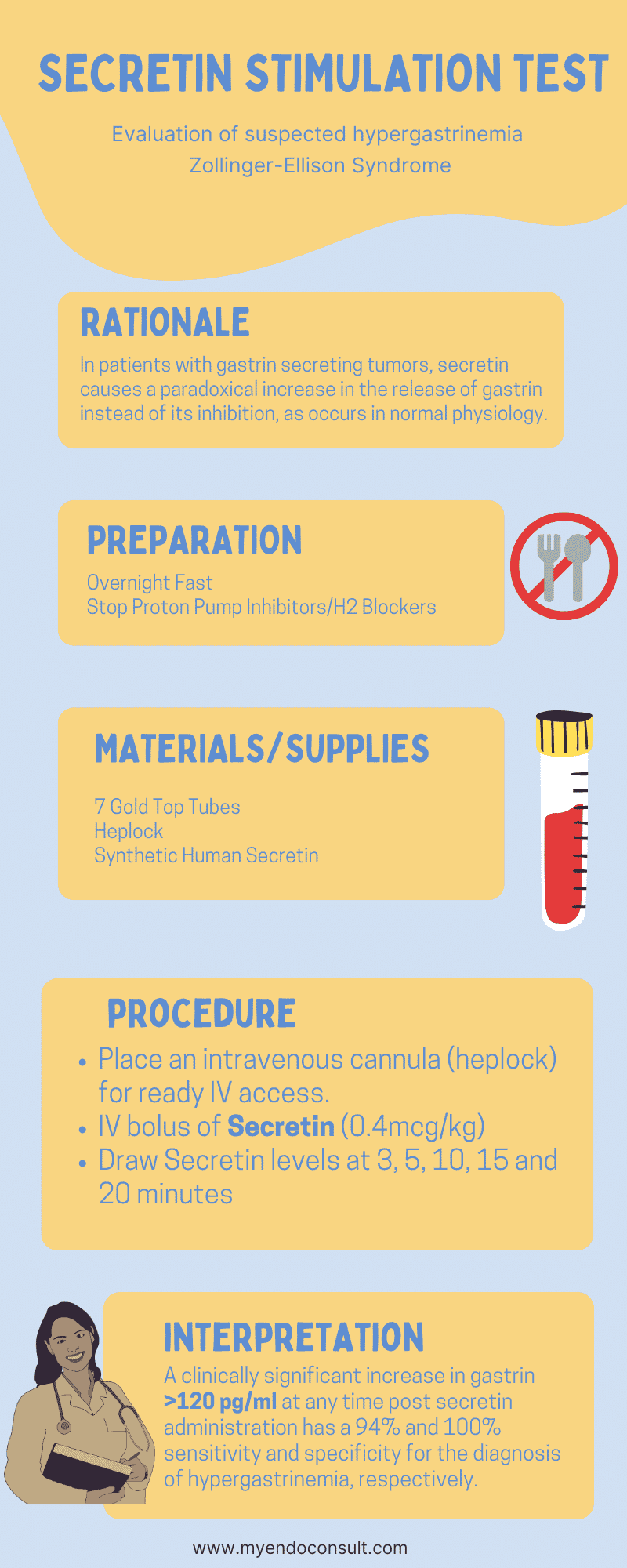
| Threshold | Sensitivity | Specificity |
| 110 pg/ml | 93% | 93%2 |
| 120 pg/ml | 94% | 100%3 |
| 200 pm/mL | 94% | 85%4 |
Due to the high specificity of 120 pg/mL cut-off (change from baseline gastrin), this is usually recommended as a diagnostic threshold for clinically significant hypergastrinemia3.
Other clinical applications of secretin stimulation testing
- The diagnosis of pancreatic insufficiency.
- Functional magnetic resonance imaging to detect defects in pancreatic secretion and possible ductal obstruction.
- Secretin is also utilized in magnetic resonance imaging of the pancreatic and biliary tree (cholangiopancreatography) to detect various congenital, neoplastic, and inflammatory conditions.
References
- Giusti, F. et al. Secretin Stimulation Test and Early Diagnosis of Gastrinoma in MEN1 Syndrome: Survey on the MEN1 Florentine Database. J. Clin. Endocrinol. Metab. 107, e2110–e2123 (2022).
- Deveney, C. W., Deveney, K. S., Jaffe, B. M., Jones, R. S. & Way, L. W. Use of calcium and secretin in the diagnosis of gastrinoma (Zollinger-Ellison syndrome). Ann. Intern. Med. 87, 680–686 (1977).
- Berna, M. J., Hoffmann, K. M., Serrano, J., Gibril, F. & Jensen, R. T. Serum gastrin in Zollinger-Ellison syndrome: I. Prospective study of fasting serum gastrin in 309 patients from the National Institutes of Health and comparison with 2229 cases from the literature. Medicine (Baltimore) 85, 295–330 (2006).
- McGuigan, J. E. & Wolfe, M. M. Secretin injection test in the diagnosis of gastrinoma. Gastroenterology 79, 1324–1331 (1980).