PHEOCHROMOCYTOMA AND PARAGANGLIOMA
Typical Duration of Spell
- Spell Duration: Commonly 15–20 minutes, but may be much shorter or last several hours.
- Important Note: Most patients with spells do not have a pheochromocytoma.
Additional Clinical Signs of Catecholamine-Secreting Tumors
- Cardiovascular
- Hypertensive retinopathy.
- Orthostatic hypotension (possible paradoxical feature).
- Angina.
- Gastrointestinal
- Nausea, constipation (megacolon can be a presenting symptom).
- Metabolic
- Hyperglycemia, diabetes mellitus (α-adrenergic inhibition of insulin release).
- Hypercalcemia (often resolves post-tumor removal, may be MEN 2–related or due to PTHrP).
- Raynaud phenomenon, livedo reticularis.
- Erythrocytosis (secondary to increased catecholamine stimulation).
- Mass Effects
- Tumor size/location effects.
- Bladder paragangliomas: Painless hematuria, paroxysmal spells triggered by micturition or defecation.
- Cosecreted Hormones
- ACTH → Cushing syndrome.
- PTH-related peptide → hypercalcemia.
- Vasopressin → SIADH.
- VIP → watery diarrhea.
- GHRH → acromegaly.
- Cardiomyopathy and Heart Failure
- Possibly unrecognized as pheochromocytoma cause.
- May be dilated or hypertrophic, often reversible post-resection.
- Myocarditis, myocardial infarction with normal coronaries also possible.
Physical Exam and Genetic Syndromes
- Possible findings from hereditary predispositions:
- Retinal angiomas, marfanoid habitus, café-au-lait spots, axillary freckling, subcutaneous neurofibromas, mucosal neuromas (e.g., MEN 2B).
- Some patients may be asymptomatic despite high catecholamine levels (receptor desensitization from chronic stimulation).
The “Rule of 10” (Historically)
- 10% are extra-adrenal.
- 10% occur in children.
- 10% are multiple/bilateral.
- 10% recur post-surgery.
- 10% are malignant.
- 10% are familial.
- 10% of benign sporadic pheos found incidentally.
(Modern data suggests up to 20% familial, and about 50% discovered incidentally in some series.)
Increasing Incidental Detection
- Widespread use of CT imaging and familial testing → up to 50% discovered before symptoms.
- Tumors found incidentally may be small (<3 cm) but can be large (≥10 cm).
Diagnosis
- Biochemical Confirmation
- Fractionated catecholamines and metanephrines (plasma or 24-hour urine).
- Imaging only after biochemical confirmation:
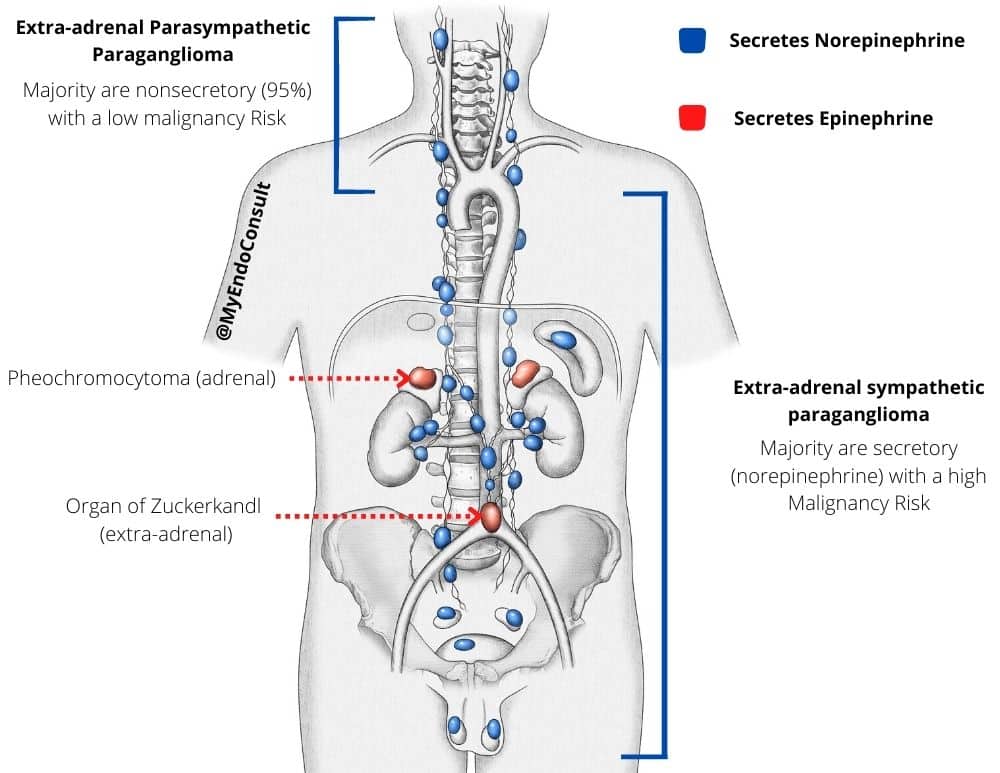
- Pheochromocytomas: Typically adrenal; average ~4.5 cm.
- Paragangliomas: Extra-adrenal chromaffin tissue (para-aortic, organ of Zuckerkandl, bladder wall, sympathetic chain in neck/mediastinum).
- Head/Neck Paragangliomas:
- Usually parasympathetic origin, nonsecretory.
- Thoracic/Abdominal/Pelvic Paragangliomas:
- Sympathetic origin, typically catecholamine-secreting.

ADRENAL MEDULLA AND CATECHOLAMINES
Anatomy and Cells
- Adrenal Medulla: Central 10% of the adrenal gland volume.
- Chromaffin Cells (Pheochromocytes): Stain brown with chromium salts (due to oxidation of epinephrine/norepinephrine).
- Sympathetic Input: Preganglionic fibers from T10–L1 splanchnic nerves.
- Stressful Stimuli: Trigger catecholamine release (MI, anesthesia, hypoglycemia).
Catecholamine Basics
- Catechol Nucleus: ortho-dihydroxybenzene ring + amino side chain.
- Epinephrine: Principal adrenal medulla hormone (80% of normal output).
- Norepinephrine: Also in adrenal medulla & peripheral sympathetic nerves.
- Dopamine: Precursor, main CNS transmitter.
Physiologic Effects
- Cardiovascular: ↑HR, BP, myocardial contractility, conduction velocity.
- Receptor Subtypes
- α1: Vascular smooth muscle contraction → ↑BP.
- α2: Presynaptic inhibition of NE release; central anti-hypertensive effect.
- β1: Cardiac inotropy, chronotropy; renin release, lipolysis.
- β2: Bronchodilation, vasodilation in skeletal muscle, glycogenolysis.
- β3: Lipolysis, energy expenditure.
- DA1 (renal vasculature dilation), DA2 (presynaptic inhibition of NE release).
Pharmacologic Implications
- Selective α/β agonists/antagonists treat various conditions (e.g., β1-blockers for HTN, α2-agonists for HTN, β2-agonists for asthma).
CATECHOLAMINE SYNTHESIS, STORAGE, SECRETION, METABOLISM, INACTIVATION
Synthesis
- Tyrosine → DOPA via tyrosine hydroxylase (rate-limiting).
- Inhibited by cytoplasmic catecholamines; relieved by secretory depletion.
- α-Methylparatyrosine (metyrosine) inhibits tyrosine hydroxylase.
- DOPA → Dopamine via aromatic L-amino acid decarboxylase.
- Dopamine → Norepinephrine via dopamine β-hydroxylase (DBH) in storage vesicles.
- Norepinephrine → Epinephrine via phenylethanolamine N-methyltransferase (PNMT) in cytosol.
- PNMT requires glucocorticoids and S-adenosylmethionine.

Storage and Secretion
- Vesicular Monoamine Transporters (VMAT): Pump catechols into secretory vesicles.
- Secretory Granules: Contain catecholamines, ATP, calcium, neuropeptides, chromogranins.
- Exocytosis Trigger: Acetylcholine (via nicotinic receptors) → depolarization → voltage-gated Ca²⁺ channels → vesicle fusion and release.
- Short Plasma Half-Life: 10–100 seconds. About half loosely bound to albumin.
Metabolism and Inactivation
- Reuptake: ~90% of synaptic NE taken up by presynaptic nerve (uptake-1); inhibited by cocaine, TCAs.
- Enzymatic: Catechol-O-methyltransferase (COMT) and monoamine oxidase (MAO) degrade catechols.
- Metanephrine/normetanephrine formed by COMT.
- Final major metabolite: vanillylmandelic acid (VMA).
- Dopamine: Metabolized to homovanillic acid (HVA).