Releasing and inhibiting hormones (via the hypophysial portal circulation) act on G-protein–linked receptors in the pituitary, altering gene transcription and hormone secretion.
Target Gland Feedback
Circulating hormones from target glands (e.g., cortisol, thyroid hormone) exert negative feedback on their respective pituitary trophic hormones.
Intrapituitary Regulation
Autocrine and paracrine cytokines/growth factors locally modulate pituitary cell development and function.
Hypothalamic Releasing/Inhibiting Hormones
Releasing Hormones: GHRH, CRH, TRH, GnRH.
Inhibitory Hormones: Somatostatin (inhibits GH) and Dopamine (inhibits prolactin).
Anterior Pituitary Hormones
Corticotropin (ACTH)
Growth Hormone (GH)
Thyrotropin (TSH)
Follicle-Stimulating Hormone (FSH)
Luteinizing Hormone (LH)
Prolactin
All are secreted pulsatilely into the systemic circulation.
Positive Feedback: The target gland hormone or a surrogate may enhance pituitary/hypothalamic release (less common).
Closed Loop vs. Open Loop:
Closed Loop: Involves only the trophic hormone and its target gland hormone.
Open Loop: Includes influence from the nervous system (emotional or external stimuli) that can adjust or override the standard feedback.
Other Factors in Feedback
Inhibin: A glycoprotein from Sertoli (testes) or granulosa (ovary) cells provides negative feedback on FSH secretion.
Endogenous Secretory Rhythms:
Circadian / Diurnal Rhythms: ~24-hour cycle.
E.g., GH and prolactin peak after sleep onset; cortisol peaks ~2–6 AM, lowest ~11 PM; testosterone highest in the morning.
Ultradian Rhythms: Occur more frequently than once a day.
Infradian Rhythms: Periods longer than a day (e.g., menstrual cycle).
Clinical Considerations
Pulsatile Secretion: A single GH measurement may not reflect overall GH status; IGF-1 is a more stable index.
Time-of-Day Reference Ranges: E.g., cortisol reference range differs between morning and afternoon blood draws.
Loss of Normal Rhythms: E.g., high midnight cortisol supports the diagnosis of Cushing syndrome (disrupted circadian rhythm).
POSTERIOR PITUITARY GLAND
Anatomy and Embryology
Neural Tissue: Formed by the distal axons of neurons in the supraoptic (SON) and paraventricular (PVN) nuclei of the hypothalamus.
Hormones Stored: Vasopressin (ADH) and Oxytocin.
Vasopressin & Oxytocin: Nonapeptides (6–amino acid ring with disulfide bridge + 3–amino acid tail).
Blood Supply: Inferior hypophysial arteries, draining into the cavernous sinus → internal jugular vein.
Storage and Release
Storage Capacity: Enough vasopressin to sustain basal release ~30 days and maximal release ~5 days.
Axonal Transport: ~90% of SON neurons produce vasopressin; the PVN also makes other peptides (somatostatin, CRH, TRH, opioids).
Secretion: An action potential from SON/PVN travels down the axon, causing Ca²⁺ influx and exocytosis of neurosecretory granules into fenestrated capillaries in the posterior pituitary.
Posterior Pituitary Bright Spot
MRI Feature: T1-weighted hyperintensity reflecting vasopressin stored in neurosecretory granules.
Absent in central diabetes insipidus.
Ectopic Location: In some congenital cases, the bright spot is found along the stalk or at the hypothalamic base; can be associated with a hypoplastic anterior pituitary and variable anterior pituitary dysfunction.
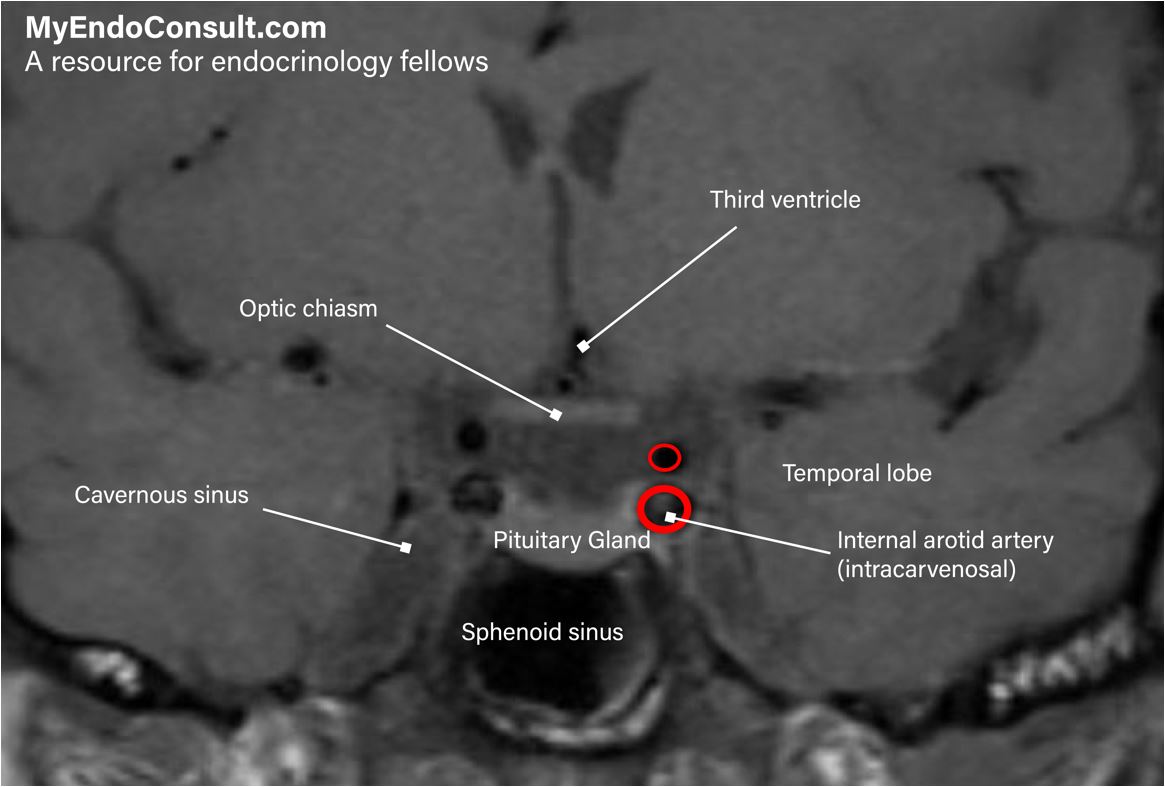
MRI of the pituitary gland (coronal section) showing its relevant anatomical relationships