Various learning theories, including cognitivist, behaviorist, and cognitivist models of multimedia learning, were implemented during the design process. Principles of instructional design were used in the development of this resource.
Introduction
There is evidence that information presented graphically enhances a learner’s understanding and decision-making ability[1]. A recent randomized controlled trial assessed the role of infographics in showcasing clinical research. Studies presented on social media via infographics had higher altmetric scores and abstract views than those presented in a text-based format[2].
Infographics were therefore selected as a medium of instruction for medical trainees interested in learning about cardinal studies in the field of endocrinology. Behaviorist and cognitivist learning theories were also applied within an instructional design model during this resource development. It was designed as a standalone resource for medical trainees with access to the internet anywhere in the world.
This aims to show medical educators the application of cognitive theories of multimedia learning within an instructional design model during the development of an infographic-based learning resource.
Overview of the resource design process
The Xerte Online Toolkit (opensource platform) and Adobe Indesign software were used for designing the resource slides and visual infographics, respectively. A storyboard served as a design sketch board during the development of this resource. The storyboard contents were then transferred to the Xerte Online Toolkit e-learning portal and tested for accuracy and ease of use at the frontend. The study resource was designed to be deployed through either a web browser on a smartphone or a desktop computer.
The instructional design model adopted for this project was the ADDIE (Analysis, Design, Development, Implementation, and Evaluation) model[3]. Behaviorist and cognitivist learning theories were implemented during the resource design and will be described later.
Instructional Design Model
The ADDIE model is widely applied in the development of curriculum in medical education[4, 5]. The steps in the ADDIE model are shown in table 1. The intended learners were defined based on the “PACT model,” an acronym for people, activity, context, and technology[6]. This model is also outlined in table 1. The target audience included medical students in their clinical years of training, internal medicine residents, and endocrinology fellows. Learners were expected to have a basic understanding of clinical trials and an ability to interpret study outcomes. They were also required to have a working knowledge of the basic statistical principles needed to assess the quality of clinical trials. Learners were introduced to selected trials in diabetes care, hypertension, hyperlipidemia, thyroid disease, and menopause.
An understanding of the general management of these conditions was required to facilitate a better appreciation of this learning resource. As adult learners, the target audience was also expected to work independently through this introductory course and willing to commit at least 60 minutes to complete all the study activities. Learners could complete this course either at home or the workplace. The learning environment, however, had to be devoid of any background noise or undue distractions to facilitate a stress-free acquisition of the core knowledge required for fulfilling the learning outcomes.
Although the PACT model served as a well-structured means of defining the learner base for this course, there was an obvious challenge. For example, the assumption that medical students in their clinical years of training should have a basic understanding of common endocrine conditions may not have been valid since they may be at varying proficiency levels with regard to medical management. For this study resource, endocrinology fellows and final year medical residents would have been a more suitable learner base since they were much more advanced in their medical education.
Table 1 ADDIE instructional design model
| Acronym | Description |
| Analysis | People (MS3, MS4 rotating through an endocrine clinic, Medical residents, and Endocrinology Fellows. Understand clinical trials and common endocrine conditions) Activity (60-minute independent learning session, One session) Context (home/workplace) Technology (Cell phone or computer with internet access) |
| Design | Storyboard (using a sketchpad and pencil) |
| Development | Xerte open-source eLearning platform (MCQs, Drag and drop quizzes and image embed features). Adobe InDesign software (designing infographics) |
| Implementation | Implementation of the learning resource. Deployed on the Cardiff Xerte design platform (https://xerte.cardiff.ac.uk/play_15079) and shared on https://www.myendoconsult.com – A collaborative learning website for endocrinology trainees. |
| Evaluation | Google feedback form (using an external link from the resource) was used in collecting learner feedback. The author performed a review of the learning resource at the front end to detect areas of improvement in usability and accessibility. |
MS3 Third-year medical student, MS4 Fourth-year medical student, MCQs multiple-choice questions
Learners were introduced to learning outcomes designed to be Specific, Measurable, Achievable, Relevant, and Timed (SMART)[7] and were required to appreciate the impact and role of landmark clinical trials in guiding the practice of medicine in general. More specifically, the knowledge acquired in this learning module was expected to allow them to solve real-world problems in diabetes care and endocrinology. In developing these study outcomes, relatively lower cognitive domains of Bloom’s taxonomy were selected, included “understanding” and “application” [8]. Other authors have cited the importance of using lower cognitive domains of Bloom’s taxonomy for independent learning experiences. Indeed, higher cognitive domains are best implemented in a more formal teaching environment[9]. These intended learning objectives were assessed in the learning resource. For example, the application of clinical trial knowledge in solving case-based problems served as a means of implementing the “application” level of Bloom’s taxonomy.
Cognitive Model of Multimedia Learning
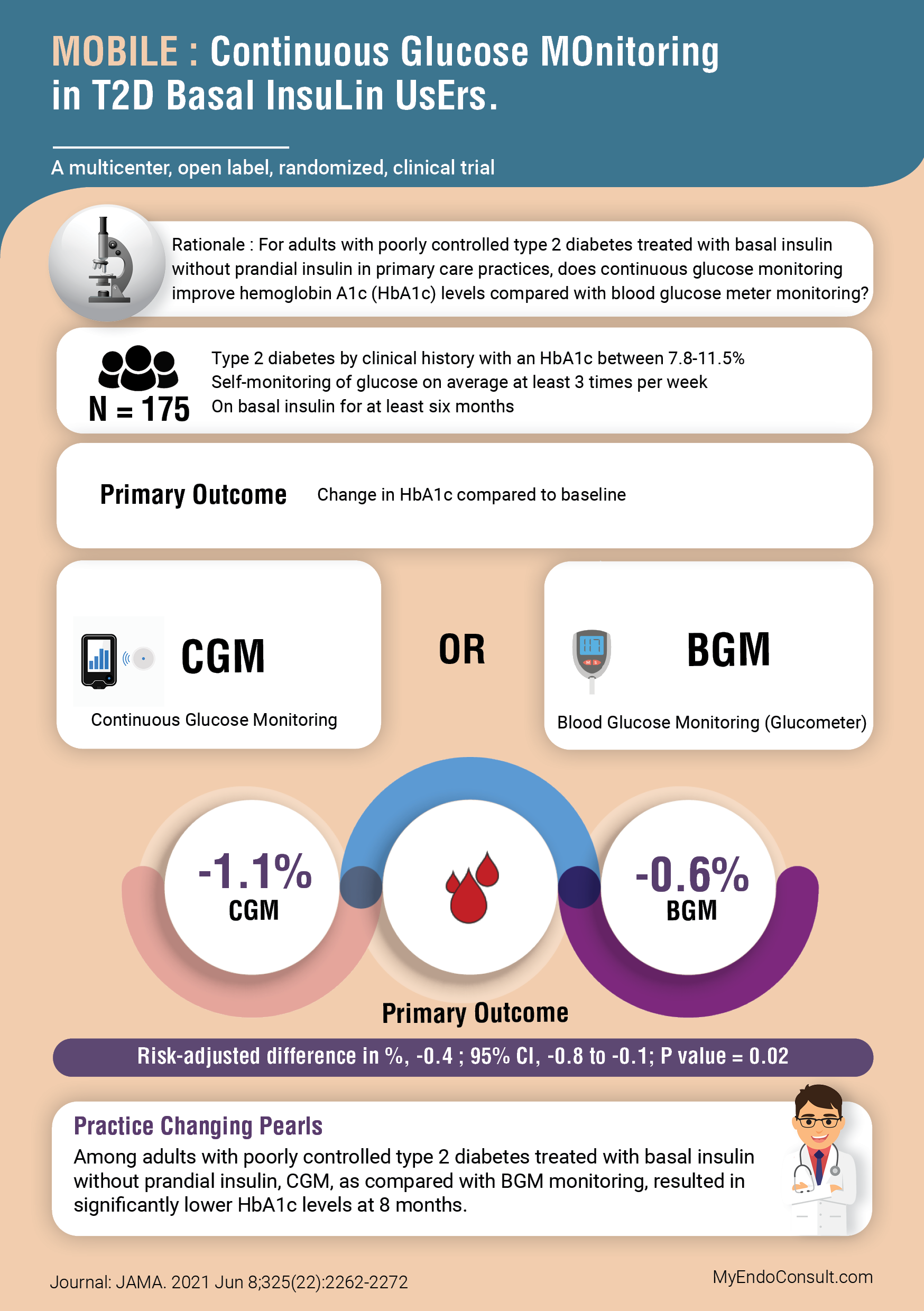
Visual infographics were selected as a more user-friendly approach to introducing trainees to complex clinical research. The trial population, interventions, and outcomes were presented in a manner that facilitated a quick review of the literature. Anecdotally, this was deemed more ideal than presenting the plain abstracts of each selected clinical trial. This approach emphasizes the cognitive theory of multimedia learning, which in effect highlights the importance of words and pictures as separate channels by which the brain processes information into working memory[10]. Each slide had a limited amount of text in order not to overwhelm the sensory perceptions of the learner. Each visual infographic could then be evaluated in its entirety by clicking on a selected acronym describing a clinical trial (see figure 1 in the appendix). A typical infographic is shown in figure 2 (see appendix).
Learning Theories
Behaviorist and cognitive learning theories informed the resource design. With regards to behaviorist learning theory, multiple-choice questions and drag and drop quizzes were used. A drag and drop “matching quiz” at the end of each set of landmark trials assessed the students’ recollection of recently acquired knowledge. This stimulus-response sequence followed by reinforcement was modeled according to a behaviorist learning theory. For example, immediate answer feedback (response) for pairings of study outcomes and acronyms (stimulus) simulated a stimulus-response chain. Wrong answers required multiple attempts, and correct answers allowed learners to proceed to subsequent sections of the resource. In effect, desired responses were reinforced by allowing students to continue. Undesired responses were extinguished by preventing students from proceeding to subsequent sections of the resource. This was intended to highlight core principles in the behaviorist learning theory[11]. Acronyms require rote memorization, a learning process that is unfortunately confined to lower levels of Bloom’s taxonomy.
Cognitivism, on the other hand, is based on a learner’s ability to acquire, process, assimilate and apply knowledge[12]. Case-based learning served as a means of assessing some study outcomes (from a cognitivist viewpoint). Learners applied both prior and recently acquired clinical trial knowledge in solving real-world problems in endocrine practice. Carefully selected real-world problems were presented in a case-based learning format. Learners were required to draw on their knowledge about these landmark trials in solving specific medical problems. Thus the selection of learners in their clinical years of training or more advanced levels of medical education. For students interested in acquiring a deeper understanding of clinical trials in the field of endocrinology, an external online study resource was provided to encourage further studies. Much higher levels of Bloom’s taxonomy could not be fulfilled in this study resource. Learners could, however, consolidate their knowledge by exploring a larger repository of clinical trials in endocrinology.
Additionally, the information processing model of cognitive psychology that emphasizes sensory, working, and long-term memories informed the design process. It is widely accepted that learning is promoted when learners are engaged in solving real-world problems and when opportunities are created for them to build on existing knowledge[13]. For this reason, integration of case-based learning scenarios in this resource facilitated assessment of learner engagement and understanding of recently acquired knowledge.
Evaluation
Learners were also given an opportunity to critique the learning resource. A graded evaluation form was modeled along the guidelines stipulated in the Learning Object Review Instrument (LORI) model [14]. Each objective was assessed via a five-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). The aim was to use relevant feedback obtained from learners in modifying the study resource for future learners. The survey is designed to last less than a minute to encourage students to provide well-needed feedback without feeling constrained by time.
Conclusion
This learning resource was designed according to a well-tested instructional design model. Also, principles in both behaviorist and cognitivist theories of education were taken into account during the design process. By deploying this learning resource via an online platform, learners in all geographic zones can have access to it. Learner feedback is intended to be collected intermittently, allowing for further improvements in the resource. In conclusion, medical educators should endeavor to implement various channels of sensory input during the design of a curriculum. Infographics, for example, can be used to simplify complex clinical trial research in a manner that draws on cognitive principles of multimedia learning and improves the acquisition of knowledge by trainees.
References
- McCrorie A, Donnelly C, McGlade K (2016) Infographics: Healthcare Communication for the Digital Age. Ulster Med J 85:71–75
- Huang S, Martin LJ, Yeh CH, Chin A, Murray H, Sanderson WB, Mohindra R, Chan TM, Thoma B (2018) The effect of an infographic promotion on research dissemination and readership: A randomized controlled trial. CJEM 20:826–833
- Allen WC (2006) Overview and Evolution of the ADDIE Training System. Advances in Developing Human Resources 8:430–441
- Battles J.B. (2006) Improving patient safety by instructional systems design. Qual Saf Health Care 15:i25–i29
- Reinbold S (2013) Using the ADDIE model in designing library instruction. Med Ref Serv Q 32:244–256
- Benyon D (2010) Designing interactive systems a comprehensive guide to HCI and interaction design, 2nd ed. Harlow : Addison-Wesley, Harlow
- Thomas PA, Kern DE, Hughes MT, Chen BY (2015) Curriculum development for medical education: A six-step approach. Johns Hopkins University Press
- Adams NE (2015) Bloom’s taxonomy of cognitive learning objectives. J Med Libr Assoc 103:152–153
- Khalil MK, Elkhider IA (2016) Applying learning theories and instructional design models for effective instruction. Advances in physiology education 40:147–156
- Mayer RE (2010) Applying the science of learning to medical education. Medical Education 44:543–549
- Lecas J-C (2006) Behaviourism and the mechanization of the mind. Comptes Rendus Biologies 329:386–397
- Torre DM, Daley BJ, Sebastian JL, Elnicki D.M. (2006) Overview of Current Learning Theories for Medical Educators. The American Journal of Medicine 119:903–907
- Merrill MD (2002) First Principles of Instruction. Educational Technology Research and Development 50:43–59
- Nesbit JC, Leacock TL (2009) Collaborative argumentation in learning resource evaluation. In: Handbook of Research on Learning Design and Learning Objects: Issues, Applications, and Technologies. IGI Global, pp 574–588