A practical approach to utilizing bone turnover markers in the management of patients with osteoporosis.
Study objectives
- Identify potential clinical applications of Bone Turnover Markers (BTMs)
- Consider pragmatic approaches for the use of BTMs with consideration of the following parameters : Variability, least significant change (LSC), reference intervals and target values.
Bone turnovers markers in research and clinical practice
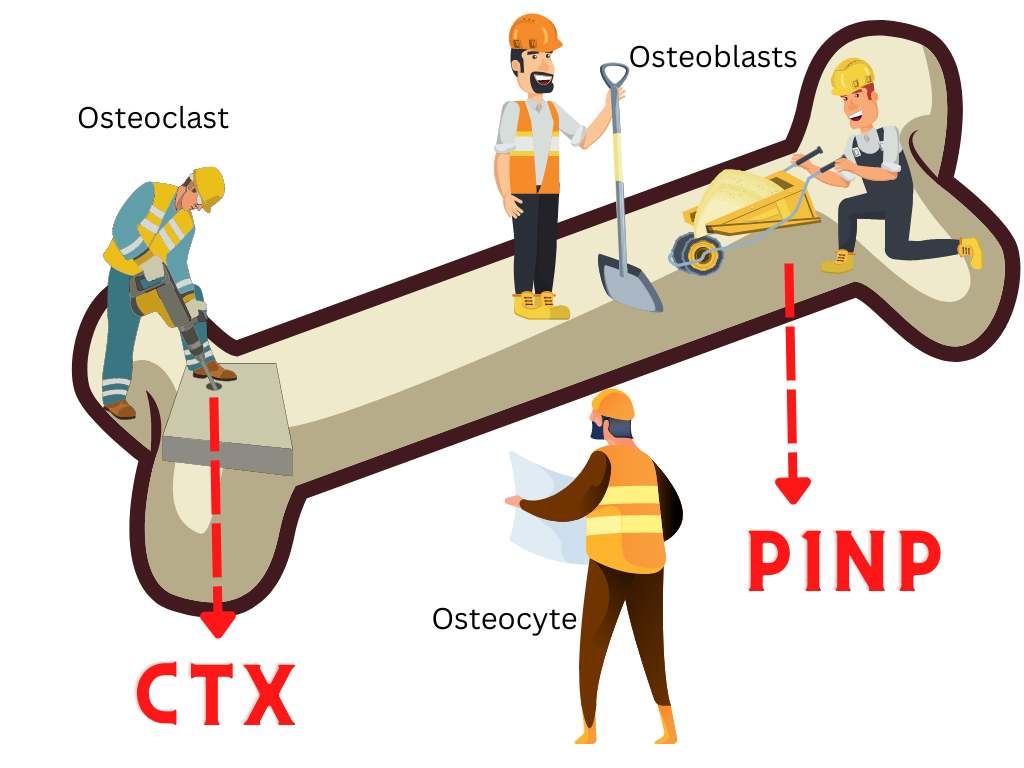
Bone resorption markers
– CTX – C-terminal telopeptide of type 1 collagen
– NTX – N-terminal telopeptide of type 1 collagen
– PYD and DPD – pyridinoline and deoxypyridinoline
– [TRACP-5b – tartrate-resistant acid phosphatase 5b]
Bone formation markers
– P1NP – N-propeptide of type 1 collagen
– P1CP – C-propeptide of type 1 collagen
– BSAP – bone-specific alkaline phosphatase
– OC – osteocalcin
Clinical application of Bone Turnover Markers
CTX represents non-helical peptide fragments of type I collagen containing cross-linking regions, released into the systemic circulation during bone resorption. It is measured in blood and urine as either ⍺-CTX (native CTX), which is not measured in commercial assays, or β-CTX (mature CTX).
Intact P1NP is a trimeric procollagen molecule produced by osteoblasts. On the other hand, total P1NP represents an assay for both intact molecule and monomeric fragments excreted by kidneys. Thus, total P1NP is likely to accumulate in CKD patients(1)
Serum CTX and P1NP are helpful for monitoring response to oral bisphosphonate therapy. Furthermore, BSAP and TRACP-5P have demonstrable utility in patients with chronic kidney disease. Reference intervals are required to interpret single values of these bone markers. For example, the median of the premenopausal reference interval is commonly used as the treatment target for antiresorptive therapy.
Serum CTX and P1NP are the preferred bone turnover markers in clinical practice. Although useful in the management of osteoporosis, it is important to note that BTMs cannot be used in specific clinical scenarios(2).
Do not use bone turnover markers for the following…
- Diagnose osteoporosis
- Predict the risk of ONJ
- Determine whether to initiate treatment with antiresorptive vs. anabolic
- Predict the rate of bone loss in individual patients
- Predict fracture risk in individual patients
When can bone turnover markers be potentially helpful?
To monitor for bone resorption during a bisphosphonate holiday. It can also be useful for monitoring increased bone resorption after discontinuation of denosumab therapy, especially after patients have been transitioned to zoledronate.
When are bone turnover markers most useful
- To monitor treatment effect with bisphosphonates, teriparatide or abaloparatide.
- To assess adherence to therapy and absorption of oral bisphosphonate therapy.
Sources of variability in bone turnover markers
As with most analytical methods in endocrinology, these can be grouped into pre-analytical, analytical and inter-laboratory.
| Source of variability | Factors |
| Pre-analytical | Age, sex, ethnicity (uncontrollable) The time of day of assessment of BTMs, timing with meals or even exercise (controllable) |
| Analytical | Precision of of the analytical method (assay) and the manner in which the specimen is processed. |
| Inter-laboratory | Highly variable with manual assays, but less with automated |
Biotin at a dose of 300mcg or more will artifactual increase serum CTX by more than 3-fold up to an hour after ingestion in some commercial assays by Roche, IDS and IDS-Isys. Biotin however has no effect on P1NP levels (Orion assay).
Also, serum CTX does increase artifactually for patients with an estmated GFR below 60. Indeed, the current KDIGO guidelines recommend against the routine utilization of CTX for patients with CKD 3a to 5. P1NP on the other hand is valid for patients with CKD.
Approaches to monitoring bone turnover markers (The Sheffield Algorithm)
The mean serum CTX in a healthy premenopausal woman is approximately 280 ng/L. The least significant change in CTX is 100 ng/L. The optimal treatment response is defined as a decrease in CTX of more than 100 ng/L to below 280 ng/L after six months of treatment [anti-resorptive therapy].
The mean serum P1NP in a healthy premenopausal woman is approximately 35mcg/L. The least significant change in P1NP is 10 mcg/L. The optimal treatment response is a decrease of more than 10mcg/L to below 35mcg/L at 6 months [anti-resorptive therapy].
Monitoring of oral antiresorptive therapy
| Time | Comments |
| Baseline | Measure either P1NP or CTX |
| 1 month | Compliance check with the patient |
| 6 months | Measure P1NP or CTX |
| 5 years | DXA to reassess fracture risk, consider BP holiday if risk is low |
The mean serum P1NP in a healthy premenopausal woman is approximately 35mcg/L. The least significant change in P1NP is 10 mcg/L. The optimal treatment response is an increase of more than 10mcg/L above 35mcg/L at 6 months [anabolic therapy].
The optimal treatment response is defined as an increase of more than 10 mcg/L at month 1 and 3 and at least 69mcg/L on one of these time points. It is worth noting that the absolute treatment target approach for P1NP is less researched than the least significant change approach.
Monitoring of anabolic therapy (teriparatide)
| Time | Comments |
| Baseline | Measure P1NP |
| 1 month | Measure P1NP |
| 3 months | Measure P1NP |
| 6 months | Repeat DXA scan |
| 2 years | Repeat DXA to establish baseline for future monitoring. Monitor P1NP. Optimal time to switch to antiresorptive (preferably a potent one like denosumab) |
A practical monitoring approach for Bone Turnover Markers
When should you order serum CTX?
- Monitor oral bisphosphonate therapy when concerned about optimal absorption and patient compliance
- Monitoring of patients on an oral bisphonphonate holiday or a long dosing interval medication like zoledronic acid.
- Monitor for rebound bone resorption when patients are transitioned from denosumab to zoledronic acid.
When should you order serum P1NP
- Monitoring all of the above scenarios (described for CTX) when insurance does not cover CTX
- Monitor response to teriparatide or abaloparatide theapy, especially when rapid feedback on treatment effect is desired.
- A change ≥ LSC in the appropriate direction (based on whether patient is on an anabolic or antiresorptive agent) is consistent with a beneficial skeletal effect.
- Treatment targets may be helpful in women but less so in men
References
- IFCC-IOF Joint Working Group on Standardisation of Biochemical Markers of Bone Turnover, Johansson H, Odén A, Kanis JA, McCloskey EV, Morris HA, et al. A Meta-Analysis of Reference Markers of Bone Turnover for Prediction of Fracture. Calcif Tissue Int. 2014 May;94(5):560–7.
- Eastell R, Pigott T, Gossiel F, Naylor KE, Walsh JS, Peel NFA. DIAGNOSIS OF ENDOCRINE DISEASE: Bone turnover markers: are they clinically useful? Eur J Endocrinol. 2018 Jan;178(1):R19–31.