Fractional Excretion of Calcium (FECa) Calculator
Fractional Excretion of Calcium (FECa): —
Important Notice for Errors
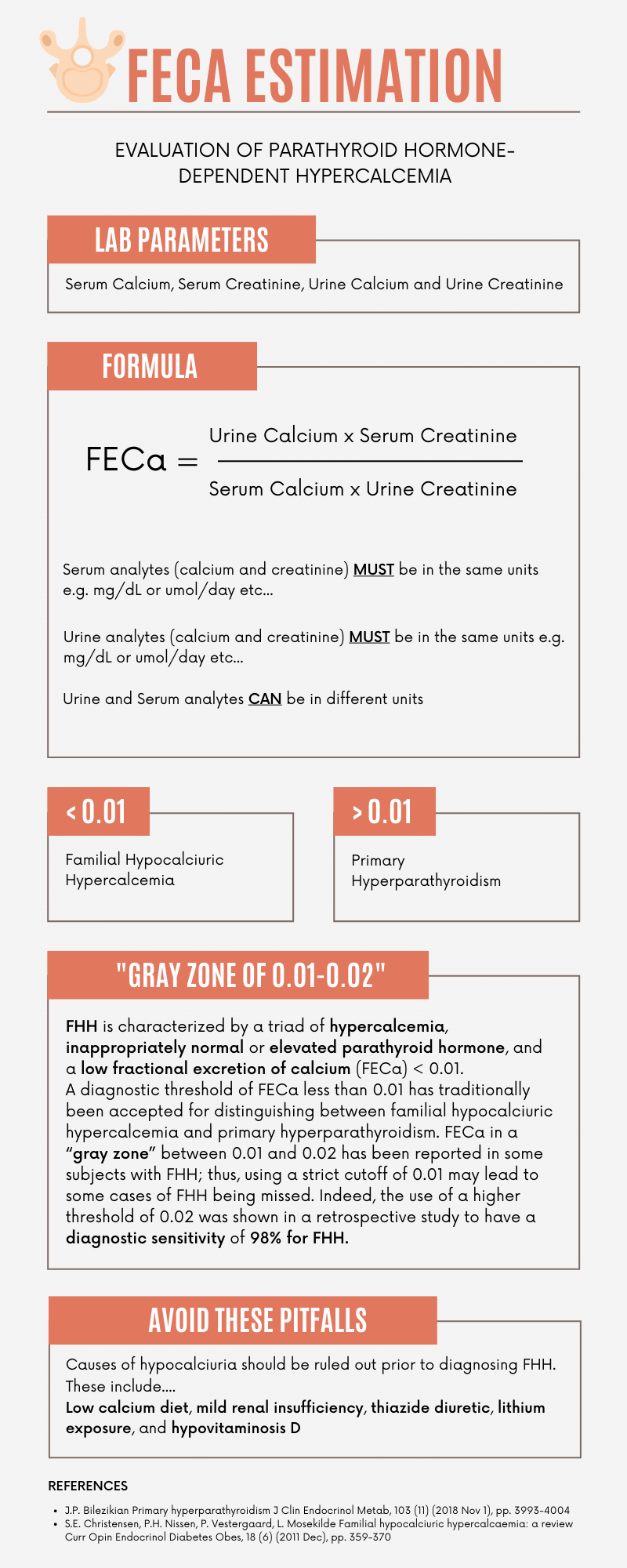
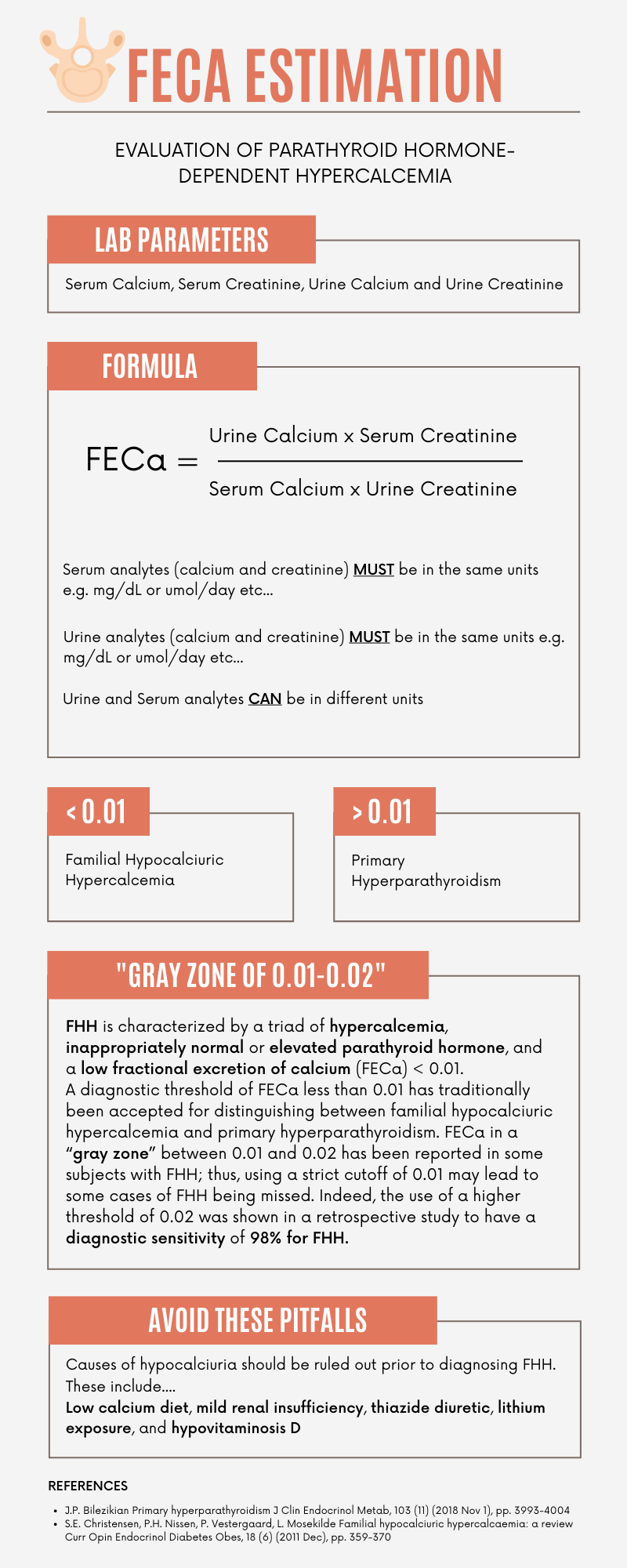
Urine calcium and creatinine need to be entered in the same conventional units (e.g. mg/dL, mmol/24hrs). If they are not the same, convert one of them to maintain consistency
Serum calcium and creatinine need to be entered in the same conventional units (e.g. mg/dL, mmol/L.). If they are not the same, convert one of them to maintain consistency.
Acceptable for serum units (e.g. mg/dL) to be different from urine units (e.g. mmol), but both serum and urine parameters should still be using the same system (US or SI)
Urine Creatinine (Please remember to change gm per 24hrs to mg per 24hrs by multiplying by 1000, for some laboratory reports)
References:
Bilezikian JP. Primary Hyperparathyroidism. J Clin Endocrinol Metab. 2018;103(11):3993-4004.
Christensen SE, et al. Familial Hypocalciuric Hypercalcaemia: a review. Curr Opin Endocrinol Diabetes Obes. 2011;18(6):359-70.
Interpretation of FECa results
> 0.01: Familial Hypocalciuric Hypercalcaemia (FHH) is unlikely. The patient most likely has primary hyperparathyroidism
< 0.01: Familial Hypocalciuric Hypercalcaemia (FHH) is likely. It is however important to rule out other causes of low urine calcium excretion such as hypovitaminosis D, low salt intake, low calcium intake, significant renal disease, lithium or thiazide diuretic exposure
Differential diagnoses of PTH dependent hypercalcemia
Download a high-resolution version (pdf print version) or picture format (PNG)
{kind=link}
The diagnostic umbrella for PTH-dependent hypercalcemia is broad, with most cases representing primary hyperparathyroidism (PHPT), after excluding other causes of hyperparathyroidism. Although a relatively rare cause of PTH-dependent hypercalcemia, misdiagnosis of a case of FHH may lead to inadvertent and possibly harmful parathyroidectomy.
FHH is characterized by a triad of hypercalcemia, inappropriately normal or elevated parathyroid hormone, and a low fractional excretion of calcium (FECa) < 0.01. A diagnostic threshold of FECa less than 0.01 has traditionally been accepted for distinguishing between familial hypocalciuric hypercalcemia and primary hyperparathyroidism. FECa in a “gray zone” between 0.01 and 0.02 has been reported in some subjects with FHH; thus, using a strict cutoff of 0.01 may lead to some cases of FHH being missed. Indeed, the use of a higher threshold of 0.02 was shown in a retrospective study to have a diagnostic sensitivity of 98% for FHH.
References
- J.P. Bilezikian Primary hyperparathyroidism J Clin Endocrinol Metab, 103 (11) (2018 Nov 1), pp. 3993-4004
- C. Brachet, E. Boros, S. Tenoutasse, W. Lissens, G. Andry, P. Martin, et al. Association of parathyroid adenoma and familial hypocalciuric hypercalcaemia in a teenager Eur J Endocrinol, 161 (1) (2009 Jul 1), pp. 207-210
- J.S. Bhangu, A. Selberherr, L. Brammen, C. Scheuba, P. Riss Efficacy of calcium excretion and calcium/creatinine clearance ratio in the differential diagnosis of familial hypocalciuric hypercalcemia and primary hyperparathyroidism Head Neck, 41 (5) (2019), pp. 1372-1378
- J.P. Bilezikian, M.L. Brandi, R. Eastell, S.J. Silverberg, R. Udelsman, C. Marcocci, et al. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the fourth international workshop J Clin Endocrinol Metab, 99 (10) (2014 Oct), pp. 3561-3569
- S.E. Christensen, P.H. Nissen, P. Vestergaard, L. Mosekilde Familial hypocalciuric hypercalcaemia: a review Curr Opin Endocrinol Diabetes Obes, 18 (6) (2011 Dec), pp. 359-370
Thank you for your positive feedback!
Great tool