Causes of pituitary stalk thickening include infiltrative conditions and tumors. A simple mnemonic for recalling the etiology is STALLC.
Causes of a thickened pituitary stalk
The pituitary stalk attaches the pituitary gland to the median eminence of the hypothalamus. The stalk is a critical transit point for hormones secreted by the neurohypophysis (posterior pituitary gland). There are both neoplastic and non-neoplastic causes of a thickened pituitary stalk.
- Langerhans Cell Histiocytosis (Histiocytosis X)
- Sarcoidosis
- Dysgerminoma
- Infundulohypophysitis
- Metastasis
- Tuberculosis
- Lymphoma
- Astrocytoma
- Infundibuloma
A simple mnemonic for thickened pituitary stalk
Causes of a thickened pituitary stalk
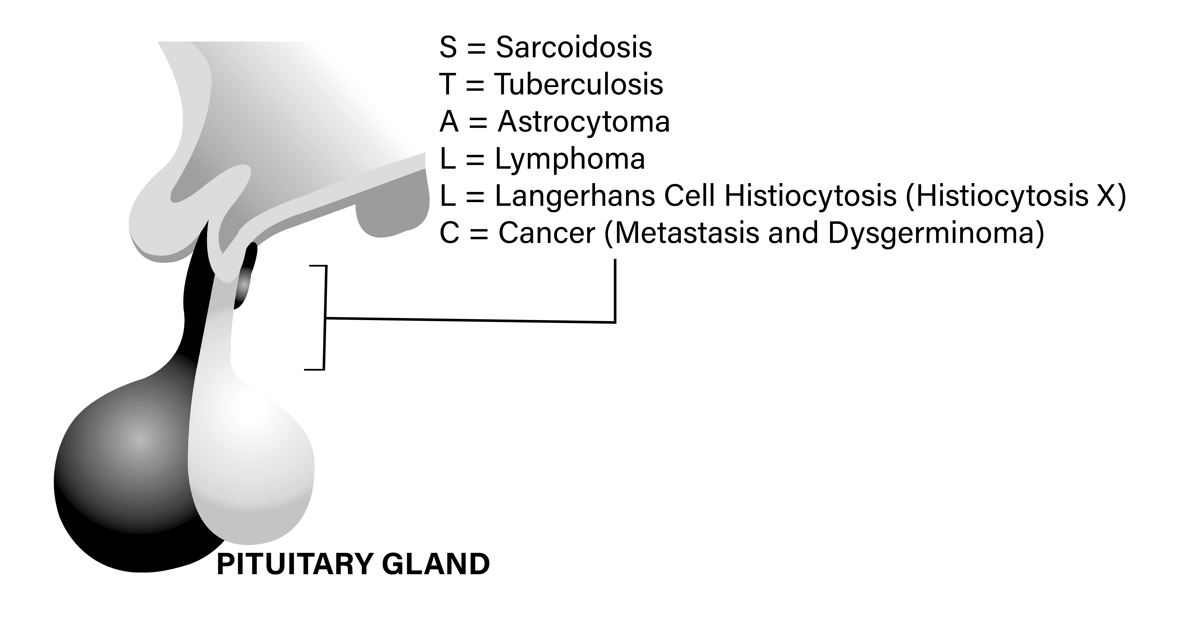
A simple mnemonic to remember this is STALLC
- S = Sarcoidosis
- T = Tuberculosis
- A = Astrocytoma
- L = Lymphoma
- L = Langerhans Cell Histiocytosis (Histiocytosis X)
- C = Cancer (Metastasis and Dysgerminoma)
Neurosarcoidosis A Cause of Thickened pituitary stalk.
A 60-year-old woman presents to the emergency department with complaints of excessive thirst, frequent urination, and dizziness for the past few days. She reports no recent fever, cough, or any other symptoms. She denies any significant past medical or surgical history, allergies, or current medications other than prednisone.
On physical examination, she is alert and oriented, but her vital signs reveal hypotension with a blood pressure of 90/60 mmHg and a pulse rate of 110 beats per minute. She has dry oral mucosa, and the skin turgor is reduced. Neurological examination reveals no focal deficits.
Laboratory investigations reveal hypernatremia with serum sodium of 152 mEq/L, serum osmolality of 320 mOsm/kg, and low urine osmolality of 100 mOsm/kg, confirming the diagnosis of diabetes insipidus. Additionally, the serum cortisol level is low at 2 µg/dL and an undetectable serum ACTH, indicating central adrenal insufficiency. Serum TSH level is 0.01 µIU/mL and a very low serum free T4, indicating central hypothyroidism.
MRI of the brain shows diffuse leptomeningeal and hypothalamic enhancement and a thickened pituitary stalk consistent with neurosarcoidosis involvement. A diagnosis of neurosarcoidosis-related diabetes insipidus and central adrenal insufficiency is made.

Figure 1.0. The pituitary stalk is thickened and demonstrates marked enhancement. (Courtesy A. Quarde MD)
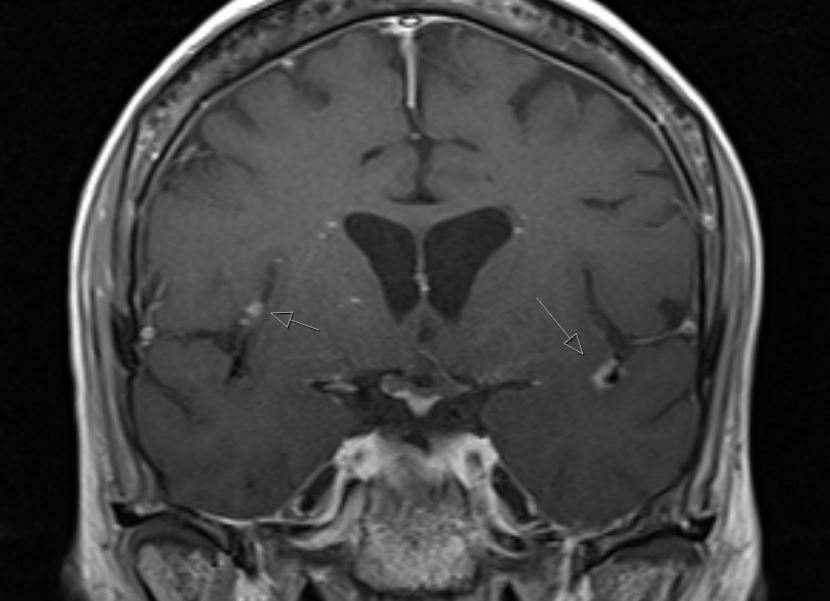
Figure 2.0. There are enhancing leptomeningeal nodules. There is partial visualization of bilateral enhancing masses near the cerebellopontine angles. There are tiny fine nodules enhancing along the pons and medulla.
The patient is started on intravenous fluids and hydrocortisone for hemodynamic stabilization. Desmopressin is administered subcutaneously for diabetes insipidus, and is admitted to the hospital for further management and monitoring. The treatment plan is coordinated with the patient’s neurologist and endocrinologist, and further investigations are planned to evaluate the extent and severity of the neurosarcoidosis involvement. She required infliximab treatment but unfortunately developed antibodies to the medication, leading to medication discontinuation. She eventually achieved remission, which was maintained with methotrexate. She understands sick day rules for steroids and is compliant with steroid replacement therapy.
References
Turcu AF, Erickson BJ, Lin E, Guadalix S, Schwartz K, Scheithauer BW, Atkinson JL, Young WF Jr. Pituitary stalk lesions: the Mayo Clinic experience. J Clin Endocrinol Metab. 2013 May;98(5):1812-8.
Images(s) Courtesy
MyEndoConsult