Prolactinomas represent the monoclonal proliferation of lactotroph cells resulting in the formation of an adenoma. Although inheritable courses of pituitary adenomas exist, such as multiple endocrine neoplasia type I, most prolactinomas occur due to sporadic mutations.
Prolactin secreting microadenomas (≤ 10 mm in largest diameter) usually present with second-degree hypogonadism (amenorrhea in women and low libido in men) with or without galactorrhea.
Macroadenomas representing tumors greater than 10 mm in size are more likely to present with mass effect symptomatology, including headaches, cranial nerve palsies, and visual field defects.
Anatomical relations of the Pituitary Gland
The hypophysis is an ovoid-shaped, reddish-gray gland measuring 12mm x 8mm in its transverse and anterior-posterior dimensions, respectively. The gland measures about 6mm in it’s cranio-caudal distance. The hypophysis sits on the floor of the sellar turcica and is bound on its superior aspect by the optic chiasm. It is bound laterally by the cavernous sinus and anterior-inferiorly by the sphenoid sinus. Finally, the gland is shielded posteriorly by the posterior wall of the sella turcica, pons, and posterior intercavernous sinus.
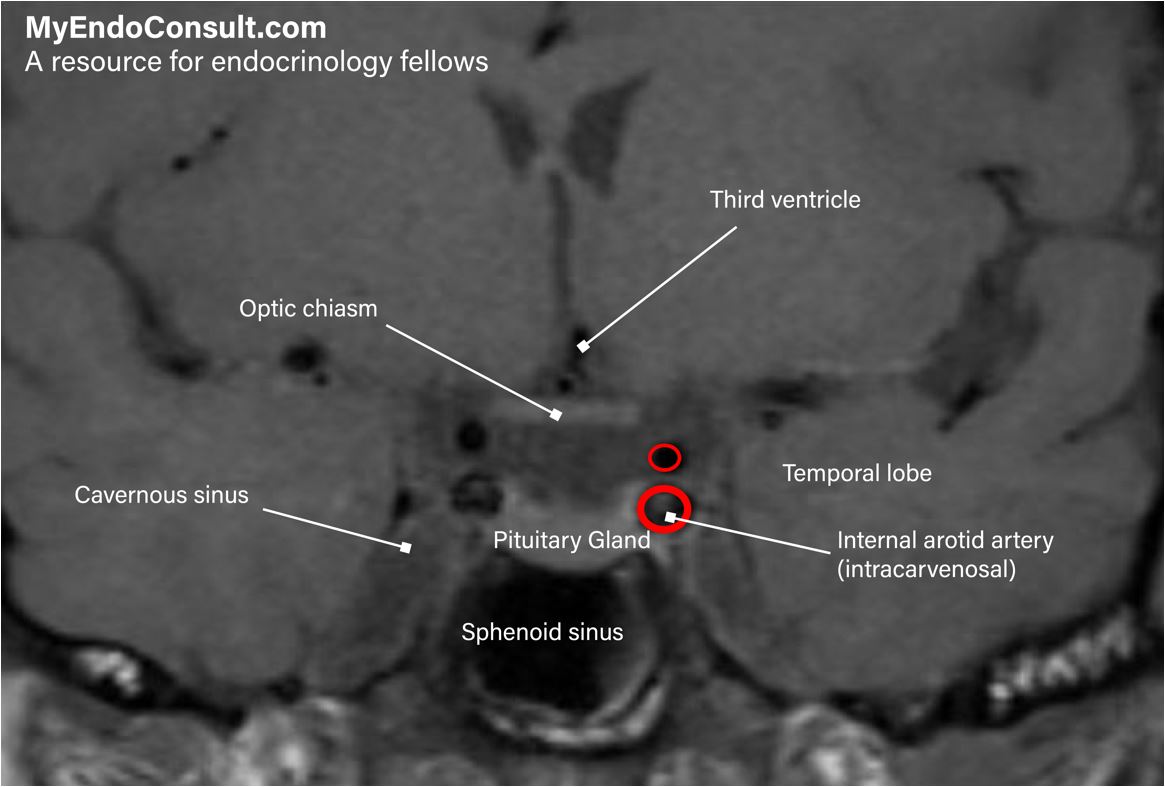
MRI of the pituitary gland (coronal section) showing its relevant anatomical relationships
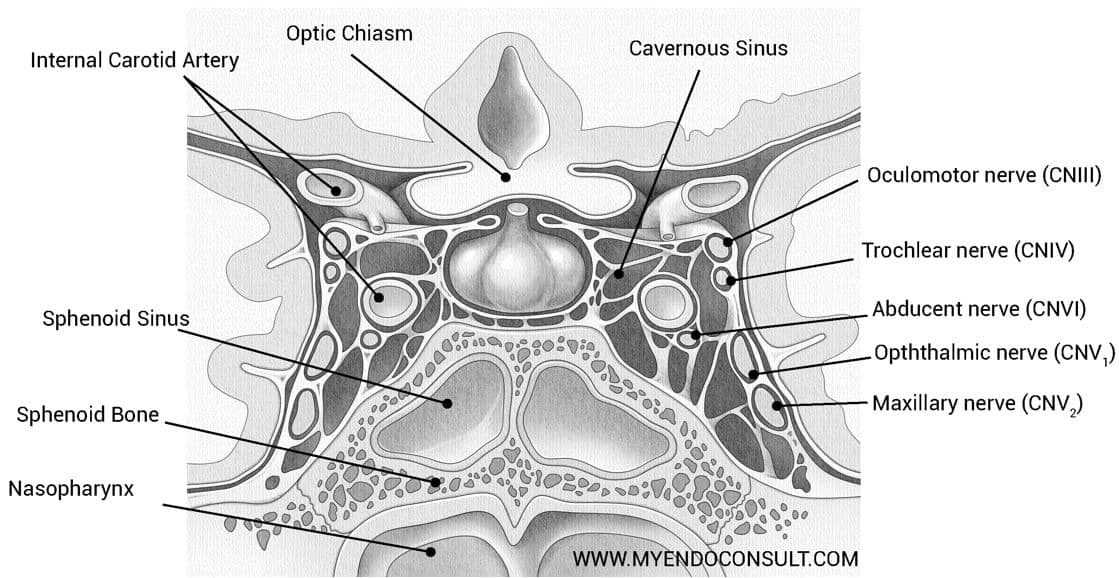
Coronal section of the pituitary gland showing the relations of the cavernous sinus to the hypophysis
MRI findings
T1-weighted magnetic resonance imaging (MRI), with coronal and sagittal images before and after administering intravenous gadolinium, is critical in identifying prolactinomas and pituitary adenomas in general. High-resolution contrast-enhanced T1-weighted images of the pituitary gland classically show a hypointense (dark) lesion consistent with an adenoma (prolactinoma). It is worth noting that normal pituitary tissue has a homogenous enhancement (brightness)on T1-weighted images1.
The signal intensity of solid prolactinomas on T2-weighted images can be used to group prolactinomas into two groups – homogeneous or heterogeneous. To estimate the T2 signal intensity of a prolactinoma, a circular region of interest (ROI) tool is utilized in comparing the tumor to gray matter (e.g., temporal gray matter. A T2 weighted intensity ratio (Tumor : Gray matter) lower than 1.0 is hypo or isointense.
Conversely, an intensity ratio >1.0 is hyperintense. Furthermore, cystic prolactinomas have unusually bright intensity on T2 weighted images2. The diagnostic yield of pituitary magnetic resonance imaging for prolactinomas increases with raising serum prolactin levels, usually above 100 ng/ml3.
Samples of prolactinomas noted on MRI
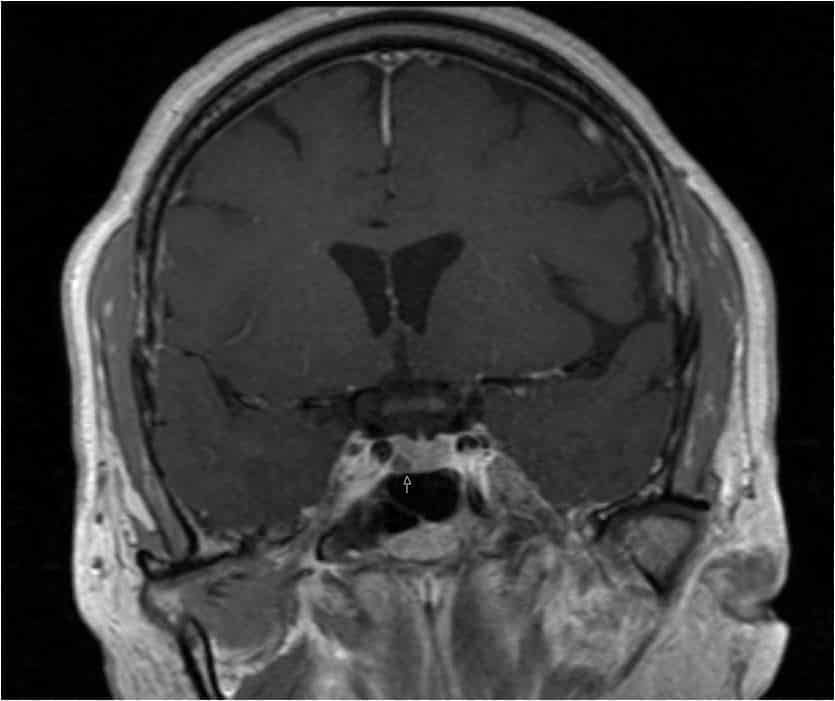
Microprolactinoma on T1-weighted images (post-gadolinium administration). The arrow shows a hypointense lesion (prolactinoma) superimposed on a hyperintense background (normal pituitary tissue). Image Courtesy (A. Quarde)
References
- Chaudhary, V. & Bano, S. Imaging of the pituitary: Recent advances. Indian J. Endocrinol. Metab. 15, S216–S223 (2011).
- Burlacu, M. C., Maiter, D., Duprez, T. & Delgrange, E. T2-weighted magnetic resonance imaging characterization of prolactinomas and association with their response to dopamine agonists. Endocrine 63, 323–331 (2019).
- Rand, T. et al. MRI of microadenomas in patients with hyperprolactinaemia. Neuroradiology 38, 744–746 (1996).