In recent years, cardiovascular disease has become one of the leading causes of death worldwide. One of the key risk factors for developing cardiovascular disease is high levels of low-density lipoprotein (LDL) cholesterol.
Estimating LDL cholesterol is essential to assessing cardiovascular risk, and several methods are available for this purpose. In this article, we will explore the different types of LDL-cholesterol and methods for estimating it in clinical practice.
What is LDL-Cholesterol?
Low-density lipoprotein cholesterol (LDL-cholesterol) is commonly known as “bad” cholesterol because elevated levels of this type of cholesterol have been linked to a higher risk of developing cardiovascular disease. LDL-cholesterol is a type of lipoprotein that transports cholesterol from the liver to cells in different parts of the body.
When LDL-cholesterol levels are high, it can result in the accumulation of plaque in the arteries, which can increase the likelihood of developing cardiovascular diseases such as heart attacks and strokes. (1)
Plaque buildup in the arteries can restrict blood flow, leading to various health problems. It is essential to maintain healthy levels of LDL cholesterol through lifestyle modifications, such as a balanced diet, regular exercise, and medication if needed.
Structure of LDL cholesterol
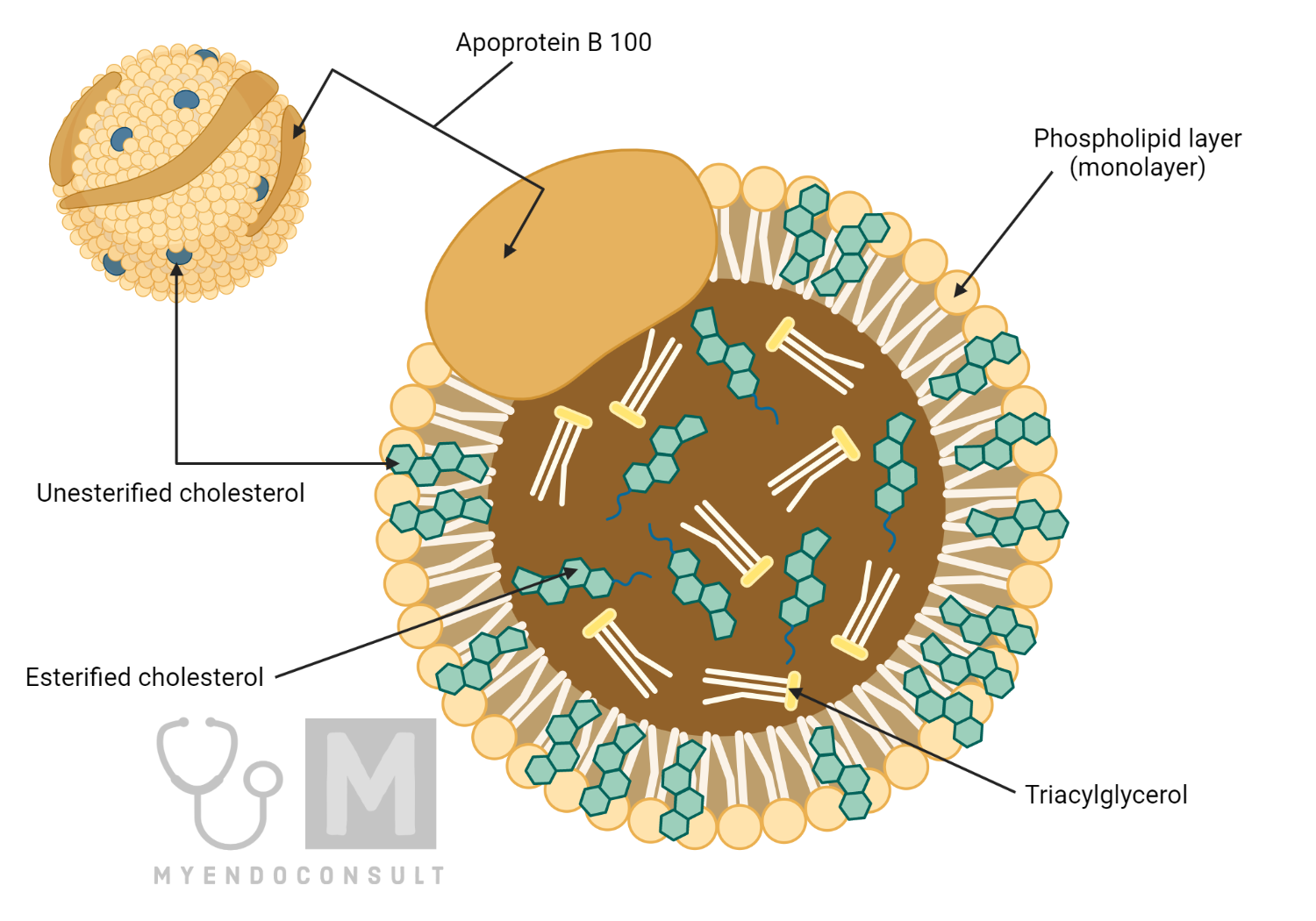
LDL (low-density lipoprotein) cholesterol is a type of cholesterol carried in the bloodstream by a complex of proteins and lipids. LDL particles comprise a core of cholesterol esters and triglycerides, surrounded by a phospholipid monolayer and several proteins, including apolipoprotein B-100 (apoB-100).
The structure of LDL cholesterol can be described as follows:
- Core: The core of the LDL particle is composed of cholesterol esters, which are formed by the esterification of free cholesterol with fatty acids. The core also contains triglycerides, composed of three fatty acids bound to a glycerol backbone.
- Phospholipid monolayer: The core of the LDL particle is surrounded by a monolayer of phospholipids, which are amphipathic molecules composed of a hydrophilic head and a hydrophobic tail. The phospholipid monolayer provides a barrier between the core of the particle and the surrounding aqueous environment.
- Apolipoprotein B-100 (apoB-100): ApoB-100 is a large protein that spans the entire length of the LDL particle. It plays a critical role in the binding and uptake of LDL particles by cells that express the LDL receptor. ApoB-100 also interacts with other proteins and lipids in the particle to help maintain its structure.
Overall, the structure of LDL cholesterol is designed to enable its transport through the bloodstream and its delivery to cells throughout the body. However, high levels of LDL cholesterol in the blood can lead to the buildup of cholesterol in the walls of arteries, which can contribute to the development of cardiovascular diseases.
Synthesis of LDL-cholesterol
LDL (low-density lipoprotein) cholesterol is a type of cholesterol that can build up in the walls of arteries and lead to various cardiovascular diseases. The body synthesizes LDL cholesterol in the liver, as well as in other tissues.
The synthesis of LDL cholesterol begins with the production of acetyl-CoA in the mitochondria of hepatic cells. Acetyl-CoA is a molecule that is produced during the breakdown of glucose or fatty acids.
Next, acetyl-CoA is converted into mevalonate through a series of enzymatic reactions, which take place in the cytoplasm of liver cells. Mevalonate is a key intermediate in the synthesis of cholesterol and other important molecules, such as isoprenoids.
Mevalonate is then converted into cholesterol through a series of enzymatic reactions that take place in the endoplasmic reticulum of liver cells. These reactions involve the sequential addition of several molecules, such as ATP and NADPH, to mevalonate.
Finally, the newly synthesized cholesterol is packaged into LDL particles in the liver and released into the bloodstream, where it can be transported to other tissues throughout the body.
It’s worth noting that the synthesis of LDL cholesterol is tightly regulated by various factors, including dietary intake of cholesterol and fats, hormonal signals, and feedback mechanisms that control the expression of key enzymes involved in the synthesis pathway. Dysregulation of LDL cholesterol synthesis can lead to high levels of LDL in the blood, which is a major risk factor for cardiovascular diseases.
Types of LDL-Cholesterol:
LDL-C can be classified into four types based on their size:
- Large (LDL I)
- Intermediate (LDL II)
- Small (LDL III)
- Very small (LDL IV)
The size of LDL particles is important because the smaller particles are more atherogenic and have a greater potential to cause atherosclerosis, which is the buildup of plaque in arteries.
The atherosclerotic plaque formation can eventually lead to coronary heart disease, stroke, and other cardiovascular diseases.
Large LDL particles are considered less atherogenic and may not contribute to the development of atherosclerosis as much as the smaller particles. On the other hand, small LDL particles are more atherogenic and have been associated with an increased risk of cardiovascular disease.
Very small LDL particles are the most atherogenic, as they can penetrate the arterial wall more easily and lead to more significant plaque formation. (2)
Measuring the size of LDL particles can be useful in predicting a patient’s risk of developing cardiovascular disease. For example, individuals with a predominance of small and very small LDL particles are at higher risk than those with a predominance of larger particles.
The measurement of LDL particle size is not routinely performed in clinical practice due to its high cost and limited availability.
The size of LDL particles plays an important role in their atherogenic potential and their contribution to the development of atherosclerosis. (3)
The measurement of LDL particle size can provide additional information about a patient’s cardiovascular risk but is not routinely used in clinical practice.
Methods of Estimating LDL-cholesterol in Clinical Practice
There are several methods for estimating LDL-cholesterol in clinical practice:
- Friedewald formula:
This formula is the most commonly used method for estimating LDL-cholesterol levels. It is calculated using the following formula:
LDL-cholesterol = total cholesterol – (HDL-cholesterol + (triglycerides / 5))
This method assumes that the triglyceride levels are less than 400 mg/dL and that the patient is in the fasting state.
However, this method may not be accurate in patients with high triglyceride levels or non-fasting patients. (4)
- Martin-Hopkins formula:
This formula is a modification of the Friedewald formula and is designed to be more accurate in patients with high triglyceride levels. (5) It is calculated using the following formula:
LDL-cholesterol = total cholesterol – (HDL-cholesterol + (0.16 x triglycerides))
- Sampson equation:
This equation uses the apolipoprotein B (apoB) levels to estimate LDL-cholesterol levels. It is calculated using the following formula:
LDL-cholesterol = (total cholesterol – HDL-cholesterol) – (0.7 x apoB)
This method may be more accurate than the Friedewald formula in patients with high triglyceride levels or non-fasting patients. (6)
- Direct LDL cholesterol assessment:
This method directly measures LDL-cholesterol levels using ultracentrifugation, electrophoresis, or a direct assay.
This method is considered the gold standard for measuring LDL-cholesterol levels, but it is more expensive and time-consuming than other methods.
Advantages and Disadvantages of Different Methods of LDL-Cholesterol Estimation
Each method of LDL-cholesterol estimation has its advantages and disadvantages. The Friedewald formula is the most commonly used method, as it is simple and cost-effective, but it is not reliable in cases where triglycerides are higher than 400 mg/dL. (7)
The Martin-Hopkins formula is more accurate and applicable to a wider range of triglyceride levels than the Friedewald formula.
It is less widely used and requires more calculations. The Sampson equation is a modification of the Friedewald formula that adjusts for the presence of intermediate-density lipoprotein (IDL) cholesterol, which can be useful in certain cases. However, it is not widely used, and there is limited research on its accuracy.
Direct LDL cholesterol assessment is the most accurate method for LDL-cholesterol estimation, as it does not rely on assumptions or calculations.It is more expensive and time-consuming than the other methods and requires specialised equipment and trained personnel. Furthermore, some studies have reported that direct LDL cholesterol assessment overestimates LDL-cholesterol levels, particularly in patients with high triglyceride levels or low HDL-cholesterol levels. (8)
| Estimation Method | Advantages | Disadvantages |
| Friedewald formula | Simple, cost-effective | Not reliable in cases where triglycerides are higher than 400 mg/dL |
| Martin-Hopkins formula | More accurate, applicable to wider range of triglyceride levels | Less widely used, requires more calculations |
| Sampson equation | Adjusts for presence of IDL cholesterol | Not widely used, limited research on accuracy |
| Direct LDL cholesterol assessment | Most accurate | More expensive, time-consuming, requires specialised equipment and trained personnel; may overestimate LDL-cholesterol levels in patients with high triglyceride levels or low HDL-cholesterol levels |
Conclusion
In conclusion, LDL cholesterol is a key risk factor for cardiovascular disease, and accurate estimation of LDL-cholesterol levels is essential for practical risk assessment and management. The Friedewald formula is the most widely used method of LDL-cholesterol estimation in clinical practice, but it has limitations, particularly in cases of hypertriglyceridemia.
The Martin-Hopkins formula, Sampson equation, and direct LDL cholesterol assessment are alternative methods that may be useful in certain cases, but each method has its advantages and disadvantages.
Clinicians should be aware of these limitations and use the most appropriate method of LDL-cholesterol estimation for each individual patient.
References
- Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972 Jun;18(6):499-502. doi: 10.1093/clinchem/18.6.499. PMID: 4337382.
- Martin SS, Blaha MJ, Elshazly MB, Toth PP, Kwiterovich PO, Blumenthal RS, Jones SR. Comparison of a novel method vs the Friedewald equation for estimating low-density lipoprotein cholesterol levels from the standard lipid profile. JAMA. 2013 Nov 20;310(19):2061-8. doi: 10.1001/jama.2013.280532. PMID: 24240933.
- Sampson M, Gopalan R, Fazio S, Linton MF. Novel methods for the measurement of HDL-C, LDL-C, and VLDL-C. Clin Lab Med. 2006 Sep;26(3):787-802, viii. doi: 10.1016/j.cll.2006.06.003. PMID: 16935240.
- Fiaschi E, Sorice GP, Sbraccia P, Paganelli M, Baldini V, Cipriano P, D’Emidio S, Silvestri A, Menichelli D, Pirro M. Evaluation of a new equation for estimating low-density lipoprotein cholesterol through the comparison with various recommended methods. Biochem Med (Zagreb). 2021 Feb 28;31(1):010701. doi: 10.11613/BM.2021.010701. PMID: 33894409; PMCID: PMC8028295.
- Jeyarajah EJ, Cromwell WC, Otvos JD. Lipoprotein particle analysis by nuclear magnetic resonance spectroscopy. Clin Lab Med. 2006 Sep;26(3):847-70, viii. doi: 10.1016/j.cll.2006.06.008. PMID: 16935243.
- Brice EJ, Murphy TP, Ikramuddin F, Wilson SA, Brethauer SA, Aminian A, Schauer PR. The impact of bariatric surgery on LDL cholesterol levels: a systematic review and meta-analysis. Surg Obes Relat Dis. 2020 Sep;16(9):1257-1264. doi: 10.1016/j.soard.2020.03.014. Epub 2020 Mar 19. PMID: 32307256.
- Kuller L, Arnold A, Tracy R, Otvos J, Burke G, Psaty B, Siscovick D, Freedman DS, Kronmal R. Nuclear magnetic resonance spectroscopy of lipoproteins and risk of coronary heart disease in the cardiovascular health study. Arterioscler Thromb Vasc Biol. 2002 Sep 1;22(9):1175-80. doi: 10.1161/01.atv.0000020482.78087.9f. PMID: 12231561.
- Nakamura T, Obata JE, Hirano M, Kodama T, Kugiyama K. Small dense low-density lipoprotein as biomarker for atherosclerotic diseases. Oxid Med Cell Longev. 2017;2017:1273042. doi: 10.1155/2017