Adenohypophysis (Anterior Lobe): Derived from oral ectoderm.
Neurohypophysis (Posterior Lobe): Derived from neural ectoderm of the forebrain floor.
Formation of Rathke Pouch (Weeks 4–5 of Gestation)
A pouch-like recess in the ectodermal lining of the stomodeum (primitive mouth).
Grows upward to meet the undersurface of the forebrain.
The connection between Rathke pouch and the stomodeum (craniopharyngeal canal) is usually obliterated.
A persistent remnant can become a “pharyngeal pituitary,” which may later give rise to ectopic hormone-secreting adenomas.
Infundibular (Neural) Outgrowth
Develops from the floor of the third ventricle (neural ectoderm).
Forms the infundibular process, which becomes solid except at its upper end (the infundibular recess of the third ventricle).
Fusion and Further Differentiation
Rathke pouch fuses with the infundibular process.
Lumen of Rathke pouch typically obliterates, but a Rathke cleft may persist.
Anterior Lobe (Pars Distalis) arises from Rathke pouch; Posterior Lobe (Pars Nervosa) arises from the infundibular process.
The neurohypophysis (posterior lobe) contains axons (about 100,000 fibers) from the supraoptic and paraventricular nuclei of the hypothalamus.
Remnants of Rathke pouch may persist at the boundary, forming small colloid cysts.
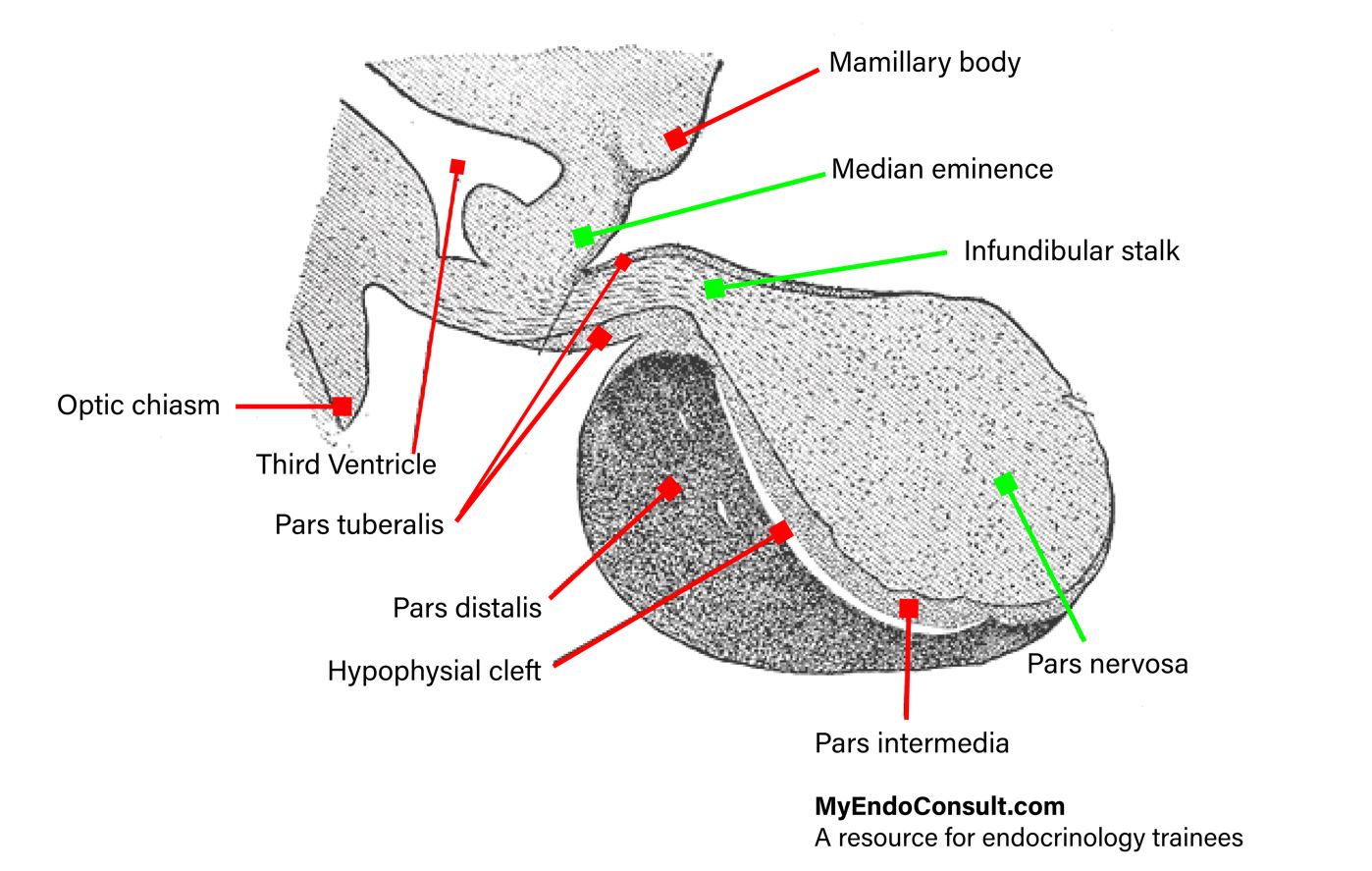
Pars Tuberalis, Pars Intermedia
The pars tuberalis extends from the ventral wall of the anterior lobe and encircles the pituitary stalk.
The pars intermedia is a thin region at the interface between the anterior and posterior lobes; in humans, it often becomes interspersed with anterior lobe cells but can produce POMC and ACTH.
The median eminence is the part of the tuber cinereum lying immediately above the pars tuberalis.
The components of the hypophysis
DIVISIONS OF THE PITUITARY GLAND AND RELATIONSHIP TO THE HYPOTHALAMUS
Adenohypophysis (Anterior Lobe)
Pars Tuberalis: Thin strip of tissue around the median eminence and upper neural stalk.
Pars Intermedia: Thin zone posterior to any persisting cleft, in contact with the posterior lobe.
Pars Distalis (Pars Glandularis): Main secretory portion.
Neurohypophysis (Posterior Lobe)
Infundibular Process (Neural Lobe)
Infundibular Stem (Neural Stalk)
Median Eminence (expanded upper end of the stalk/tuber cinereum)
Pituitary Stalk
Formed by the infundibular stem plus surrounding parts of the adenohypophysis (pars tuberalis).
Approximately 15% of the neurohypophysis extends up the stalk into the median eminence.
Nerve Supply (Hypothalamohypophysial Tract)
Main functional/anatomical supply of the neurohypophysis.
Supraopticohypophysial Tract: Arises in the supraoptic and paraventricular nuclei; runs in the anterior (ventral) wall of the stalk.
Tuberohypophysial Tract: Arises in the dorsal/posterior hypothalamic regions, including paraventricular nucleus and tuberal/mamillary areas.
These fibers terminate mainly in the neurohypophysis.
Damage above the median eminence affects ~85% of the supraoptic/paraventricular neuron cell bodies; damage at the level of the diaphragma sellae affects ~70% of these cells.
Hypothalamic Boundaries
Anteroinferiorly bounded by the optic chiasm/tracts, posteriorly by the posterior perforated substance and cerebral peduncles, and separated from the thalamus by the hypothalamic sulcus.
Merges anteriorly with preoptic septal region and posteriorly with the midbrain tegmentum.
Connective Tissue Trabecula
Separates the anterior and posterior lobes internally for a variable distance, forming part of the vascular bed.
The embryonic cleft (Rathke pouch remnant) may persist in this trabecula, more easily seen in newborns and often disappears with age.
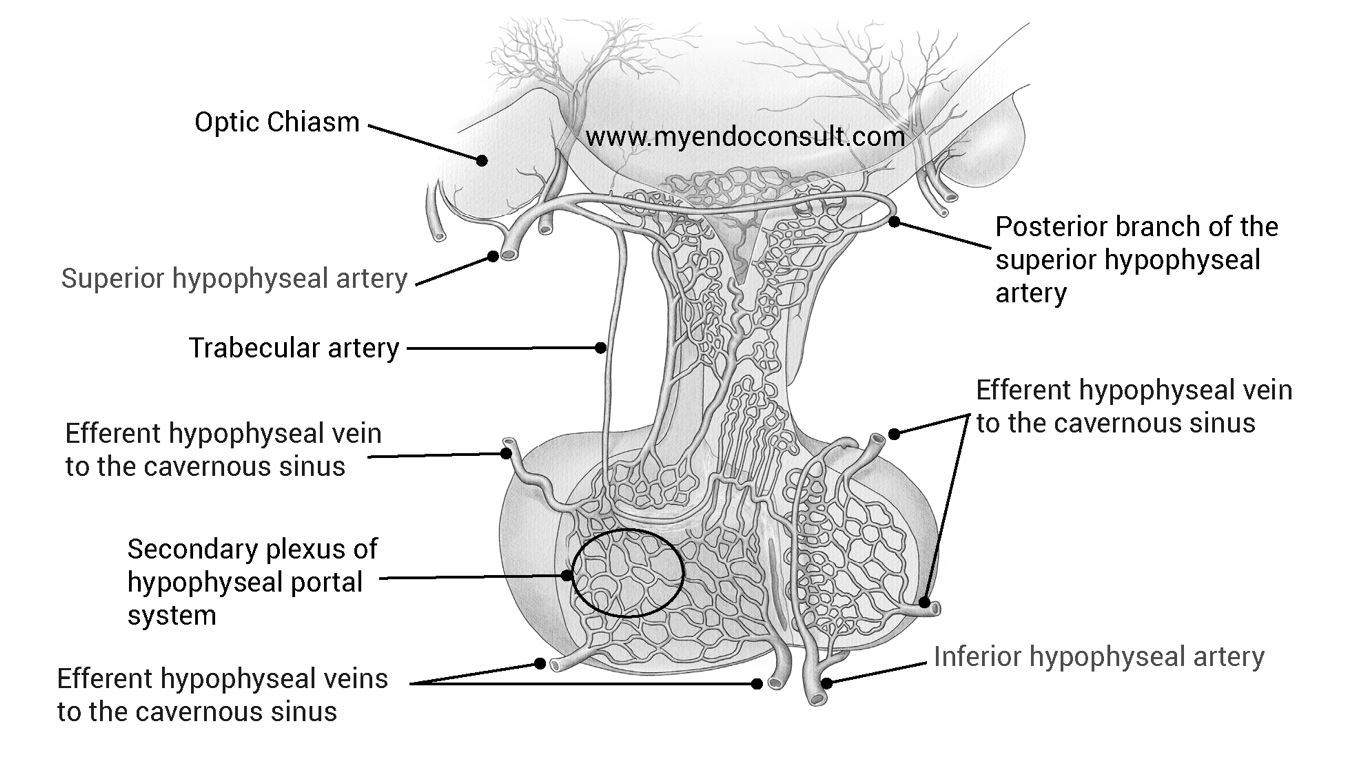
BLOOD SUPPLY OF THE PITUITARY GLAND
Arterial Supply
Superior Hypophysial Arteries (right and left) arise from the ophthalmic or internal carotid artery segment.
Each divides into anterior and posterior branches to the pituitary stalk.
Artery of the Trabecula: A branch supplying the connective tissue trabecula in the anterior lobe.
Inferior Hypophysial Arteries (right and left) branch from the intracavernous segment of each internal carotid artery.
Surround the infundibular process with an arterial ring.
Supply the posterior lobe and lower infundibular stem.
Hypophysial Portal System
Primary Capillary Network in the median eminence and infundibular stem receives hypothalamic releasing and inhibiting hormones from nerve endings.
Long and Short Hypophysial Portal Veins:
Convey blood (and hypothalamic hormones) from the primary capillary network to the secondary plexus of sinusoids in the anterior lobe (pars distalis).
The anterior lobe has no direct arterial supply; it relies on these portal vessels.
Venous Drainage flows from the secondary plexus into dural sinuses around the pituitary, then into general circulation.
Occlusion of these portal vessels can lead to ischemic necrosis of the anterior pituitary.
Venous and arterial supply of the pituitary gland. AH adenohypophysis, NH neurohypophysis
ANATOMY AND RELATIONSHIPS OF THE PITUITARY GLAND
Size and Position
Reddish-gray, ovoid organ measuring ~12 mm (transverse), 8 mm (AP), 6 mm (vertical).
Weighs ~500 mg in men and ~600 mg in women.
Sits in the hypophysial fossa of the sphenoid bone, beneath the diaphragma sellae (a dura mater fold).
The floor of the hypophysial fossa is part of the roof of the sphenoid sinus.
Diaphragma Sellae
Pierced by a small aperture for the pituitary stalk.
Separates much of the pituitary gland from the optic chiasm.
The subarachnoid space may extend partially into the sella (“partially empty sella”) and can allow blood or CSF to enter this space.
Hypothalamus
Lies superiorly, forming the floor and lateral walls of the third ventricle.
Mamillary bodies mark the posterior limits of the hypothalamus.
The optic chiasm lies just anterior/superior to the pituitary stalk and diaphragma sellae.
Optic Chiasm
A flat, quadrilateral bundle of optic nerve fibers at the junction of the anterior wall of the third ventricle with its floor.
Rests on the diaphragma sellae behind the optic groove of the sphenoid bone.
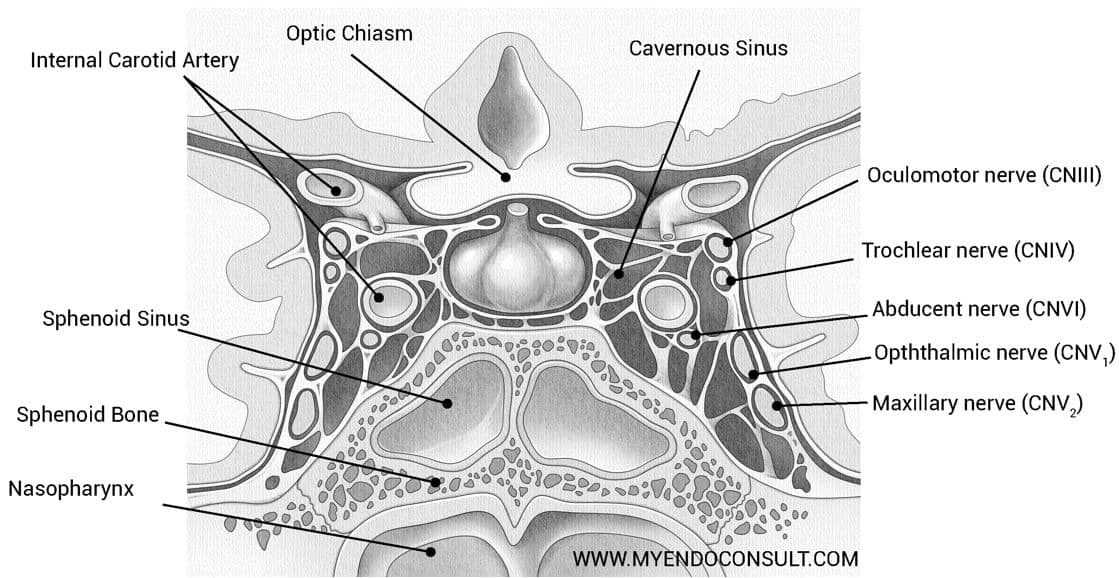
Superior Petrosal Sinus: Connects cavernous sinus to the transverse sinus; runs in the attached margin of the tentorium cerebelli.
Inferior Petrosal Sinus: Also connects cavernous sinus to other posterior dural sinuses.
Internal Carotid Artery (Intercavernous Portion)
Curves upward, forward, and then upward again through the cavernous sinus.
Perforates the dura of the sinus roof near the anterior clinoid process.
Surrounded by sympathetic fibers.
Gives off hypophysial arteries to supply posterior lobe and median eminence (portal system).
RELATIONSHIPS OF THE SELLA TURCICA
Location and Dimensions
A deep depression in the body of the sphenoid bone.
Normal adult dimensions:
AP length <14 mm
Height <12 mm (floor to a line from tuberculum sellae to posterior clinoid tip)
Sphenoid Bone Overview
Composed of a median body and two pairs of wings (greater and lesser), plus two pterygoid processes.
Sphenoidal Air Sinuses: Large cavities within the body, separated by a septum (often oblique).
Superior surface articulates with the ethmoid and frontal bones; houses grooves for the olfactory bulbs, and the chiasmatic sulcus for the optic chiasm.
Key Features
Tuberculum Sellae: A raised area behind the chiasmatic sulcus.
Dorsum Sellae: Posterior boundary of the sella turcica, ending in the posterior clinoid processes.
Hypophysial Fossa: Deepest part, housing the pituitary gland.
Clivus: A shallow depression behind the dorsum sellae, leading to the basilar part of the occipital bone.
Lateral aspects relate to the cavernous sinus and the foramen lacerum region.
Nasal Relations
The crest of the sphenoid bone and the perpendicular plate of the ethmoid.
Surgical Considerations
Modern pituitary approaches (microscopic or endoscopic) aim to avoid major vascular structures and the optic pathways.
Transsphenoidal surgery exploits the sphenoidal sinus route to access the sella turcica.