Overview of Calcitonin
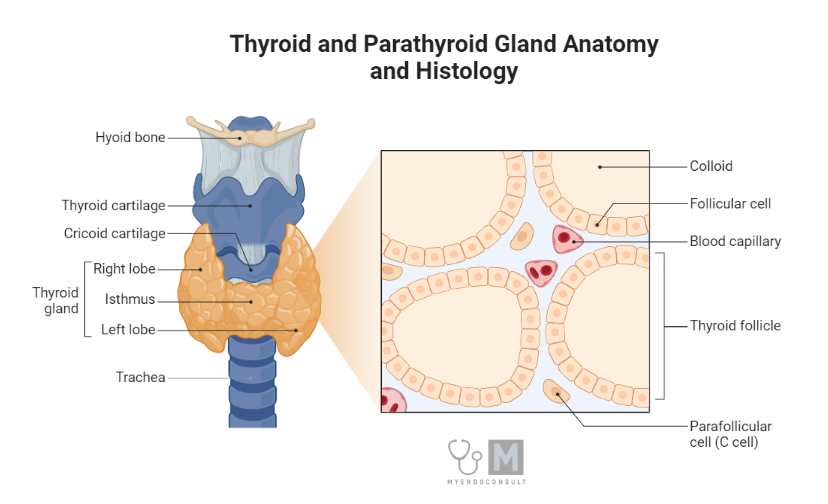
Calcitonin is a hormone comprised of a 32-amino-acid peptide chain released from the parafollicular or ‘C’ cells of the thyroid gland. This hormone originates from larger precursor peptides known as pre-procalcitonin and procalcitonin. It resides in the secretory vesicles of the parafollicular cells until it is released through a process called exocytosis.
Along with calcitonin, some procalcitonin and a dual form of calcitonin, both inactive, are also released. For calcitonin to have considerable biological activity, its entire amino acid sequence is necessary. However, the structures of calcitonin differ notably among humans and animals, such as pigs, cows, and sheep. Interestingly, the most active calcitonin molecules are found in fish and birds.
Regulation of Calcitonin Release
The primary regulator of calcitonin release from ‘C’ cells is the concentration of free ionized calcium in the blood. An increase in blood calcium levels stimulates the release of calcitonin, while a decrease inhibits it. This is opposite to the effect of calcium on the secretion of parathyroid hormone (PTH).
The gastrointestinal hormone gastrin also promotes the release of calcitonin, potentially providing a feedback mechanism to prevent high blood calcium levels after eating. Calcitonin’s presence in the blood is relatively short-lived due to the rapid breakdown of the peptide in the plasma and kidney.
Key Actions of Calcitonin
Unlike PTH, calcitonin reduces calcium levels in the plasma. It achieves this primarily by:
- Reducing the release of calcium across the bone membrane from osteocytes to osteoblasts, and by inhibiting bone resorption. It does this by directly suppressing osteoclast bone cell activity and reducing the formation of new osteoclasts from bone marrow precursors. Calcitonin’s effects are more potent when bone resorption rates are high.
- Restricting the reabsorption of calcium and phosphate in the renal tubules. Calcitonin doesn’t significantly affect calcium levels in the intestines.
Though calcitonin’s effects generally counteract those of PTH, it isn’t considered as critical as PTH and vitamin D in the usual regulation of calcium or skeletal stability in humans. Calcitonin influences target tissues, like osteoclast cells, by interacting with specific surface membrane receptors associated with intracellular cAMP production. The regions of the kidney tubule that respond to calcitonin are distinct from those responding to PTH.
Clinical Conditions Associated with Calcitonin
Clinical disorders linked to either excessive or insufficient calcitonin are uncommon. However, certain types of medullary thyroid carcinomas, which originate from parafollicular ‘C’ cells or abnormal tumors in other areas like the lungs or breasts, can trigger excessive secretion of calcitonin.
In such situations, there isn’t a significant imbalance in plasma calcium and phosphate levels, but the surplus calcitonin can be a useful tumor marker. Similarly, the removal of the thyroid gland due to thyrotoxicosis does not lead to extreme hypercalcemia.
Therapeutic Applications of Calcitonin
Calcitonin is primarily used therapeutically in the treatment of severe Paget’s disease of bone and the management of severe hypercalcemic states:
- Paget’s disease is a prevalent chronic condition of unknown cause (possibly viral) that impacts about 0.5% of individuals, particularly men, over the age of 40. The disease is marked by an unusually high level of bone turnover due to excessive osteoclastic bone resorption followed by heightened activity of osteoblasts trying to repair the bone damage. Despite increased bone turnover, the condition is initially largely symptom-free. Plasma calcium and phosphate levels remain normal, though an elevated level of alkaline phosphatase may be present, indicating osteoblastic cell activity and bone turnover.
Common symptoms include joint and bone pain, fractures, and bone deformities — particularly affecting the legs and skull, leading to auditory and optic nerve compression. Pig-derived calcitonin or synthetic salmon calcitonin may be administered daily via subcutaneous or intramuscular injection for several months to reduce bone resorption, improve bone abnormalities, and relieve bone pain and neurological complications associated with the disease.
Other medications are also available for treatment, such as bisphosphonates. These compounds reduce osteoclastic bone resorption and are absorbed strongly into bone crystals, slowing their formation and dissolution. They also indirectly inhibit osteoclast cell activity by decreasing the production of osteoclast-stimulating factors by osteoblasts.
- In hypercalcemic states, pig-derived calcitonin or synthetic salmon calcitonin can be used to produce a rapid reduction in the plasma calcium concentration in some patients with hypercalcemia. However, long-term use of calcitonin over several months can lead to clinical resistance due to a down-regulation of calcitonin receptors on target tissues. In cases of severe hypercalcemia, slow intravenous infusion of bisphosphonate drugs are also now widely used in the control of tumor-induced hypercalcemia of malignancy.
Conclusion
Understanding the role of calcitonin in the body, specifically, its impact on calcium and phosphate balance, provides a vital foundation for diagnosing and treating various medical conditions. Although disorders directly linked to calcitonin are rare, it can still serve as a critical biomarker in identifying certain carcinomas. The therapeutic applications of calcitonin, particularly in managing Paget’s disease of bone and severe hypercalcemic states, highlight its clinical importance.
As researchers continue to unravel the intricacies of this hormone, they can explore novel therapeutic approaches for managing not only bone health but also other potential areas influenced by calcitonin. Hence, ongoing research and clinical studies are pivotal for a comprehensive understanding of this hormone and the potential therapeutic opportunities it offers.
References
Davey RA, Findlay DM. Calcitonin: physiology or fantasy? J Bone Miner Res. 2013 May;28(5):973-9.
Chesnut CH 3rd, Azria M, Silverman S, Engelhardt M, Olson M, Mindeholm L. Salmon calcitonin: a review of current and future therapeutic indications. Osteoporos Int. 2008 Apr;19(4):479-91