In this article, we will review an increasingly rare example of an iodine deficiency disorder known as cretinism.
What is cretinism
The term cretin describes mentally deficient subjects born in an endemic goiter area, which exhibit some of the following characteristics which are not readily explained by other causes:
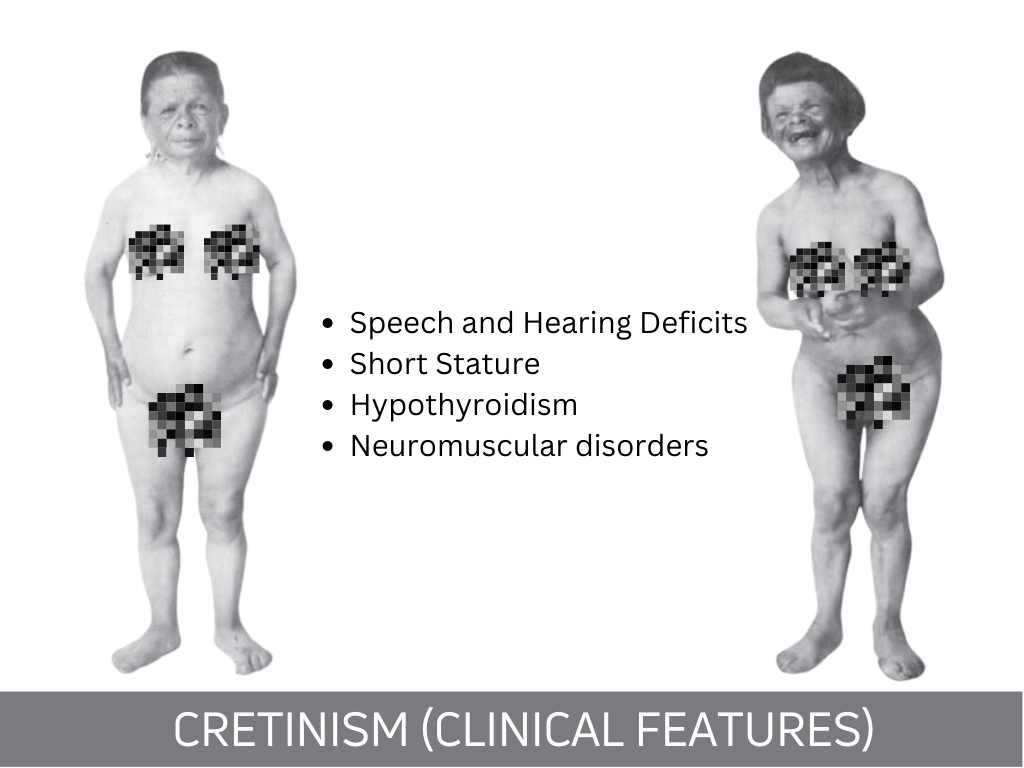
- Irreversible neuro-muscular disorders.
- Irreversible abnormalities in hearing and speech, which sometimes lead to deaf mutism.
- Impairment of somatic development.
- Hypothyroidism.
Thus, the only constant clinical feature of cretinism is a mental deficiency; in its absence, the diagnosis is hard to accept. All other symptoms may be present in very variable degrees, which, although all cretins look somehow like siblings, gives each cretin some individuality.
In very mild cases the diagnosis can only be suspected and there are no clear-cut criteria or laboratory tests by which borderline cases can be separated from normal persons.
The difference between Congenital athyrotic hypothyroidism and cretinism.
Congenital athyrotic hypothyroidism and endemic cretinism are difficult to differentiate. Although there is an overlap of many symptoms, differentiation is generally possible on clinical grounds.
While the endemic cretin is born as such, with irreversible damage to the hearing organ and the brain; mental and physical development is only slightly retarded in the congenitally athyrotic child.
A subject with congenital athyrotic hypothyroidism has a height which is near-normal in most cases, although bone maturation is delayed. Furthermore, these patients have an alertness that is reduced, but there are no hearing loss or other signs of neurologic damage.
Thyroid hormone substitution therapy is of little value in improving the central nervous system manifestations of endemic cretinism, although some effect on growth, skeletal maturation, and the development of puberty is possible.
In contrast, much depends on early thyroid hormone replacement therapy in congenitally hypothyroid children, and the brain damage can often be kept to a minimum. However, when left untreated, congenitally hypothyroid children come to resemble endemic cretins more and more over time.
Prevalence of cretinism.
Endemic cretinism occurs only in areas where goiter is severely endemic. It is never observed near the sea coast. Historically, cretinism has been familiar for centuries in the Alps (Savoy, Piedmont, Steiermark, Salzburg area), in the Pyrenees, the Carpathian mountains, the Caucasus, southern Sweden, Hungaria, and Yugoslavia. During the previous century, endemic cretins had been detected and well studied in many parts of Asia (Himalayas, Sumatra), Africa (Uele, Idjwi Island), and New Guinea (Mulia valley), and in parts of the South American Andes (Gujas, Brazil; Ecuador; Peru).
The incidence of cretinism is very difficult to estimate in a given focus of endemicity because the symptomatology is so variable. Certainly, case reports of cretinism are infrequent.
Etiology and pathogenesis of cretinism
Endemic cretinism only occurs in areas of severe iodine deficiency. The urinary iodine excretion (roughly equal to the iodine intake) is under 15 mcg per day in most areas where cretins are born. As in the case of endemic goiter, goitrogenic compounds of food and drinking water may also play some part. Mothers of endemic cretins always have a goiter and have lived in an area where it is endemic at least during pregnancy. On endemicity, cretinism is often clustered within a few families. However, hereditary factors certainly play only a minor role. Interestingly, mothers who have given birth to several cretins have normal children after moving to a village where the condition is not endemic; conversely, families who move into an endemic focus have the same incidence of cretinous children as the native population.
The exact pathogenesis of cretinism remains unknown. The most likely mechanism is that the iodine deficiency interferes with the early function of the fetal thyroid gland. Between the 80th and 90th days of fetal development, follicular lumina appear in the previously solid thyroid tissue, and thyroglobulin and hormone synthesis get underway. At approximately the same time, TSH and thyroxine become detectable in fetal blood. The concentration of thyroxine in the maternal circulation bears little relation to the concentration in the fetal circulation, and the fetus is dependent on its own hormone production and receives little hormone from the mother. Even if the dietary iodine available were enough to maintain borderline euthyroidism in the mother, the fetus might pass through a phase of perhaps only slight hypothyroidism. At a critical time, this could cause irreversible damage to the developing central nervous system. In later fetal life, lack of thyroid hormone predominantly affects growth and bone maturation.
These changes are reversible by thyroid hormone replacement. This theory is rendered less acceptable by the fact that fetal thyroid hormone lack due to other causes (such as thyroid aplasia) does not produce deafness or irreversible brain damage. Several children in whom hormone replacement was started during the first days of life almost universally go on to have normal mental development. Only if left untreated do such children become retarded and finally resemble true endemic cretins, but even then, nerve deafness is an infrequent finding.
Alternative mechanisms have therefore been proposed. Some authors think the damage to the inner ear takes place in very early pregnancy, before there is any discernible fetal thyroid function. The assumption is that an iodinated compound different from thyroid hormone is necessary for normal maturation of the central nervous system. In summary, the pathogenesis of the neurologic deficits of cretinism is only partly explained by a lack of fetal thyroid hormone. Other mechanisms must also be involved.
Clinical Features of Endemic Cretinism
The severity of cretinism is best graded by the degree of mental retardation. In mild cases, the patients are able to talk, read and write and can perform simple tasks. Mild cretins have married and have had children. Moderate cases are capable of communicating with other people with the aid of gestures and a few words. They can only perform very simple work. Severely affected patients are completely hard of hearing and incapable of any work and, in most cases, need permanent care in nursing homes.
Cretins often have a very typical appearance, and they have been distinguished from other forms of developmentally challenged subjects for centuries. They have a round face, generally with an amiable serene expression. The slow growth of the skull base with persistent synchondrosis between the sphenoid and occipital bone produces the depressed nasal bridge with apparent protrusion of the cheek and jaw.
The hairline is low, the scalp hair is coarse and fur-like, beard growth is sparse, and the skin is wrinkled and myxedematous. In typical cases, the diagnosis can be made on the spot. In any area, most cretins look like siblings from one big family. Cretins do not look young, nor does age show upon them. This classic description of the “alpine” type is not applicable to cretins in the Andes, New Guinea, the Himalayas, and Africa, where neurologic symptoms often predominate.
Mental and neurologic damage can assume any degree of severity. The decreased intelligence, combined with affective and emotional changes and with hypothyroidism, produces a characteristic psychological picture. Cretins are good-humored, sometimes even witty. The sexual drive is diminished in most cases, although occasionally, cretinous women have conceived children. The incidence of deafness varies greatly from one focus of endemicity to the other (Table 16). Deafness is primarily of neurologic origin (sensorineural hearing loss), but middle-ear changes due to faulty bone development are also a contributory factor.
Speech can be totally deficient or reduced to a few badly articulated sounds. In mild cases language is quite well developed but the vocabulary remains limited, and the voice retains a monotonous intonation. Mental deficiency is by definition a feature of endemic cretinism.
The degree of short stature is variable and is dependent on the severity of hypothyroidism, and goitrous cretins with normal thyroid function are often of normal height. As in congenital hypothyroidism, short stature is disproportioned, with short extremities. Skull size is small in absolute terms, but is normal relation to the subject’s height.
Many signs of endemic cretinism are dependent on the degree of concomitant hypothyroidism. Due to motor incoordination, muscular weakness, and cretinous dysplasia, cretins have a slow waddling gait. Spasticity of the legs may occasionally make cretins incapable of walking.
The skin is often thickened, dry, and scaly, as in simple myxedema (hypothyroidism), sometimes with a brownish hue. After puberty, myxedematous skin changes often regress and leave a coarse wrinkling which, especially on the forehead, contributes much to the typical appearance of cretins.
There are cretins with goiter and cretins without goiter. The latter are usually severely cretinous, tend to be hypothyroid, and are shorter in stature. The thyroid gland may be completely atrophic and be replaced by a few fibrous nodules. In such cases hypothyroidism is very frequent.
Differential Diagnosis of cretinism
In classic adult cases the Diagnosis is easy, but in the newborn it can be quite difficult. Children with endemic cretinism have to be differentiated from congenitally hypothyroid children with thyroid aplasia.
Prognosis of cretinism
With good care, life expectancy is virtually normal. Thyroid carcinoma is more frequent in cretins, but the cretinous state is not associated with an increased risk of any other potentially lethal diseases.
Prevention and Treatment
Prevention is achieved by the same means as that of endemic goiter. Endemic cretinism is eradicated much more rapidly and easily than endemic goiter. Worldwide, populations with a high prevalence of cretinism have seen a dramatic decline in its incidence since the introduction of iodinated salt.
Treatment of cretins is challenging. Much of the central nervous system damage is irreversible when the cretins are first seen. It is possible that early thyroid hormone substitution could improve the outcome, as in sporadic congenital hypothyroidism. In later life, thyroid hormone replacement may improve the state of hypothyroid cretins slightly.
Error in the first caption: iodine, not iron.