
Thyrotoxicosis and Hyperthyroidism : What is the difference?
Thyrotoxicosis is a clinical syndrome characterized by a hypermetabolic state resulting from elevated levels of free thyroxine (T4) and/or triiodothyronine (T3) in the blood. It is important to distinguish thyrotoxicosis from hyperthyroidism, as the two terms are not synonymous. Hyperthyroidism refers specifically to an overproduction of thyroid hormones due to increased biosynthesis and secretion by the thyroid gland, as seen in conditions like Graves’ disease and toxic nodular goiter. On the other hand, thyrotoxicosis may also arise from non-synthetic causes, such as the release of stored hormones during thyroiditis or excessive intake of exogenous thyroid hormones.
Interestingly, elevated levels of free thyroid hormones do not always manifest as clinical thyrotoxicosis. For example, in the syndrome of Resistance to Thyroid Hormone (RTH), mutations in the thyroid hormone receptor beta (TRβ) lead to tissue-specific resistance. This resistance results in decreased thyroid hormone action in tissues predominantly expressing TRβ, such as the liver and pituitary, while tissues expressing mainly thyroid hormone receptor alpha (TRα), like the heart, may exhibit symptoms of thyrotoxicosis.
The most common cause of thyrotoxicosis is Graves’ disease, an autoimmune disorder that involves stimulating antibodies targeting the TSH receptor. However, this condition represents just one of many possible etiologies. Understanding the underlying cause of thyrotoxicosis is critical for selecting appropriate treatment and ensuring effective management.
Causes of Thyrotoxicosis
The etiologies of thyrotoxicosis can be divided into two main categories: those associated with hyperthyroidism and those occurring without hyperthyroidism.
A) Thyrotoxicosis With Hyperthyroidism
- Graves’ disease is the most common form, driven by TSH receptor-stimulating antibodies that lead to diffuse thyroid overactivity.
- Toxic adenoma and toxic multinodular goiter arise from autonomously functioning thyroid nodules caused by somatic mutations in the TSH receptor or related pathways, leading to unregulated hormone production.
- Hyperthyroid thyroid carcinoma and familial non-autoimmune hyperthyroidism are rare causes involving mutations that enhance thyroid hormone synthesis.
- TSH-secreting pituitary adenomas result in inappropriate stimulation of the thyroid by excessive TSH.
- Gestational hyperthyroidism, often transient, is triggered by high levels of human chorionic gonadotropin (hCG) acting on TSH receptors, especially in early pregnancy or with trophoblastic tumors like choriocarcinoma.
B) Thyrotoxicosis Without Hyperthyroidism
- Thyroiditis, including subacute, silent, and drug-induced forms, results from the release of preformed thyroid hormones due to glandular inflammation or injury.
- Exogenous thyroid hormone intake (thyrotoxicosis factitia) occurs when individuals consume excessive doses of thyroid hormones, often either iatrogenically or for weight loss.
- Struma ovarii, a rare ovarian tumor composed of thyroid tissue, can occasionally cause hyperthyroidism if the ectopic thyroid tissue becomes functional.
Toxic Adenoma: A Key Cause of Thyrotoxicosis
Toxic adenoma, a monoclonal thyroid nodule that functions independently of TSH, produces excessive amounts of T4 and/or T3. This condition leads to suppression of TSH and often results in thyrotoxicosis. The prevalence of toxic adenoma is higher in iodine-deficient regions and among women. Larger nodules, especially those exceeding 3 cm, and older patients are at greater risk for developing overt hyperthyroidism.
Patients with toxic adenoma typically present with symptoms of thyrotoxicosis such as weight loss, tremors, and palpitations. Unlike Graves’ disease, features like exophthalmos and pretibial myxedema are absent. Diagnosis involves laboratory confirmation of suppressed TSH and elevated thyroid hormones, alongside imaging studies. Thyroid scans show focal uptake in the nodule with suppressed surrounding tissue, distinguishing it from diffuse uptake seen in Graves’ disease.
Management of Toxic Adenoma
Treatment options for toxic adenoma include:
- Radioactive iodine therapy (RAI), which targets the nodule to reduce its activity and size. However, hypothyroidism may occur in some cases due to collateral damage to surrounding tissue.
- Surgical excision, especially in cases of large nodules, symptomatic compression, or patient preference. Preoperative preparation with antithyroid drugs and beta-blockers is often required.
- Percutaneous ethanol injection offers a less invasive alternative, inducing necrosis of the nodule and improving thyroid function.
Toxic Multinodular Goiter
In toxic multinodular goiter, multiple autonomous nodules within the thyroid contribute to excessive hormone production. This condition is more common in older adults and iodine-deficient regions. The clinical presentation includes typical thyrotoxic symptoms, and in severe cases, compressive signs such as dysphagia or hoarseness due to the enlarged gland.
Diagnosis relies on thyroid function tests and imaging studies, which reveal uneven nodular uptake. Treatment mirrors that of toxic adenoma, with surgery or RAI being the definitive options. Cross-sectional imaging may be required in cases of significant gland enlargement or airway compression.
Graves’ Disease
Hyperthyroidism, also known as thyrotoxicosis, is often a result of an overactive thyroid gland, which is commonly associated with an autoimmune condition called Graves’ disease. In patients with this condition, the bloodstream carries specific thyroid-stimulating immunoglobulins (TSIs) that attach to the TSH receptors on the thyroid’s follicular cells, stimulating them to produce thyroid hormone just like natural TSH does.
Autoantibodies against thyroglobulin and thyroid peroxidase may also be present. Graves’ disease is more prevalent in women aged 40 to 50, being five to eight times more common than in men, and it frequently co-occurs with other autoimmune disorders such as myasthenia gravis, Addison’s disease, and pernicious anemia.
Key symptoms of Graves’ disease include:
- High basal metabolic rate—this leads to a general increase in body metabolism; more heat production causes heat intolerance, excessive sweating, and warm skin.
- Weight loss despite normal or increased appetite as a result of muscle wasting; other symptoms can include diarrhea and menstrual irregularities.
- Rapid heart rate, trembling, palpitations, and other types of fast heart rhythms (atrial fibrillation in elderly people), and high blood pressure. These symptoms are often due to increased thyroid hormone secretion, which enhances the responses of the sympathetic nervous system, as a result of an increase in the number and affinity of β-adrenergic receptors.
- Psychological symptoms include restlessness, anxiety, nervousness, irritability, hyperexcitability, and emotional instability.
- Changes in eye appearance—in about half of the patients, the eyelids may retract and eyeballs may protrude (known as exophthalmos or proptosis) due to swelling of the muscles surrounding the eyes. This is caused by the infiltration of lymphocytes and the deposition of mucopolysaccharides and fluid in the soft tissues around the eyes.
- Diffuse toxic goiter, which is a symmetrical enlargement of the thyroid gland.
- Elevated levels of thyroid hormones (T3 and T4) in the bloodstream, while the serum TSH level is low or undetectable due to excessive negative feedback effects of the high T3/T4 hormones on the anterior pituitary gland.
Differential Diagnoses of Hyperthyroidism
Toxic Multinodular Goiter. This condition is often seen in older patients due to the growth of several hyperactive thyroid nodules. Initially, the patient may exhibit normal thyroid hormone levels, but these nodules start operating autonomously over time, resulting in mild hyperthyroidism without exophthalmos. As relapses are frequent after antithyroid drug treatment, the standard treatment generally involves surgery or radioactive iodine. The root cause of this condition remains unknown.
Solitary Toxic Nodule. This situation can arise in patients of any age when a single overactive thyroid nodule (such as a benign autonomous follicular adenoma not controlled by the pituitary) secretes excessive thyroid hormones. Patients usually exhibit mild hyperthyroid symptoms and might be treated with radioiodine or partial thyroidectomy.
Subacute Thyroiditis (De Quervain’s Thyroiditis). This is a relatively rare, self-limiting inflammation of the thyroid, likely caused by a virus, which can occur after an upper respiratory tract infection. Depending on the severity of the inflammation, patients may experience thyroid swelling, tenderness, and pain while swallowing. Hyperthyroid symptoms like weight loss, excessive sweating, irritability, rapid heart rate, and tremors might also appear due to the inflammatory release of preformed thyroid hormone. The treatment involves oral pain relievers, corticosteroids for thyroid pain and inflammation, and propranolol for hyperthyroid cardiac effects. A temporary phase of mild hypothyroidism might follow the condition.
Thyrotoxic Crisis (Thyroid Storm). This is an uncommon but severe medical emergency triggered by a sudden release of large quantities of thyroid hormone in a hyperthyroid patient otherwise under control following sudden stress, infection, or after surgery/radioiodine treatment in unprepared patients. Symptoms include extreme restlessness, confusion, abdominal pain, rapid heart rate (possibly leading to heart failure), and fever. Immediate treatment involves propranolol (administered via slow intravenous infusion), antithyroid drugs, and aqueous iodine (either orally or via a nasogastric tube if necessary) alongside corticosteroids, antibiotics, and intravenous fluids/electrolytes.
Secondary hyperthyroidism can also develop from the following scenarios:
- Deliberate consumption of excessive amounts of thyroid hormone in an effort to lose weight (Thyrotoxicosis factitia).
- A pituitary adenoma that produces TSH (rare).
- An ovarian teratoma with thyroid components (Struma ovarii).
- Metastatic thyroid carcinoma (of the follicular type).
- Treatment with the cardiac anti-arrhythmic drug amiodarone.
The TRH test can be an effective tool in diagnosing hyperthyroidism. In this test, a dose of 400 μg of TRH is administered intravenously, and the plasma levels of TSH are measured both before and approximately 20-30 minutes after the injection to examine the anterior pituitary’s appropriate response. In patients with primary hyperthyroidism, the anticipated increase in plasma TSH, typically between 5-30 mU/l, is suppressed due to the ongoing negative feedback inhibition of the pituitary by high levels of thyroid hormones. For some patients, the injection of TRH may result in a temporary rise in blood pressure, increased heart rate, or bronchospasm.
Algorithm for Evaluating Hyperthyroidism
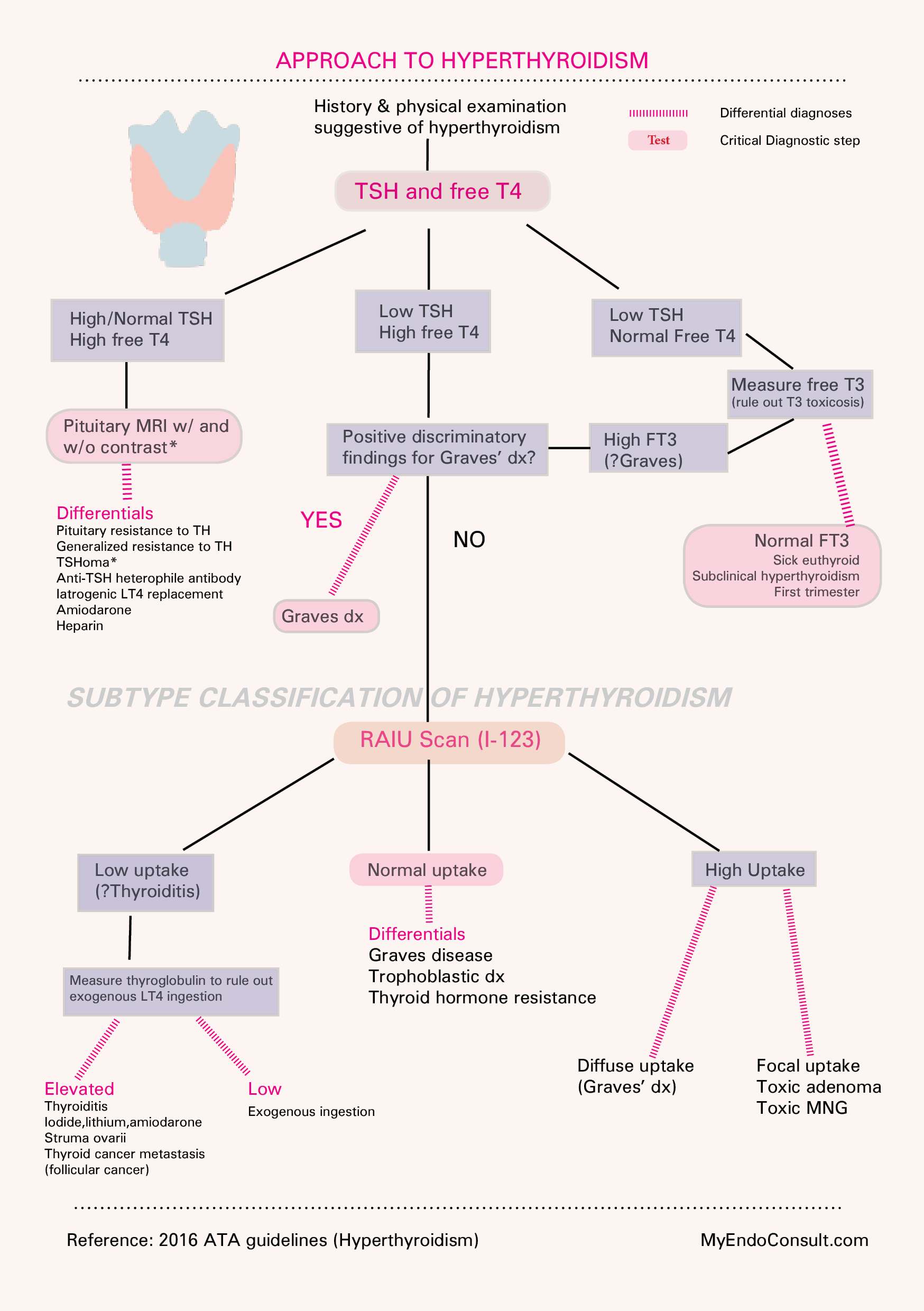
Evaluation of hyperthyroidism (An Algorithm-based approach)