Skip to content January 11, 2025
Aldosteronism Home › 4 min read
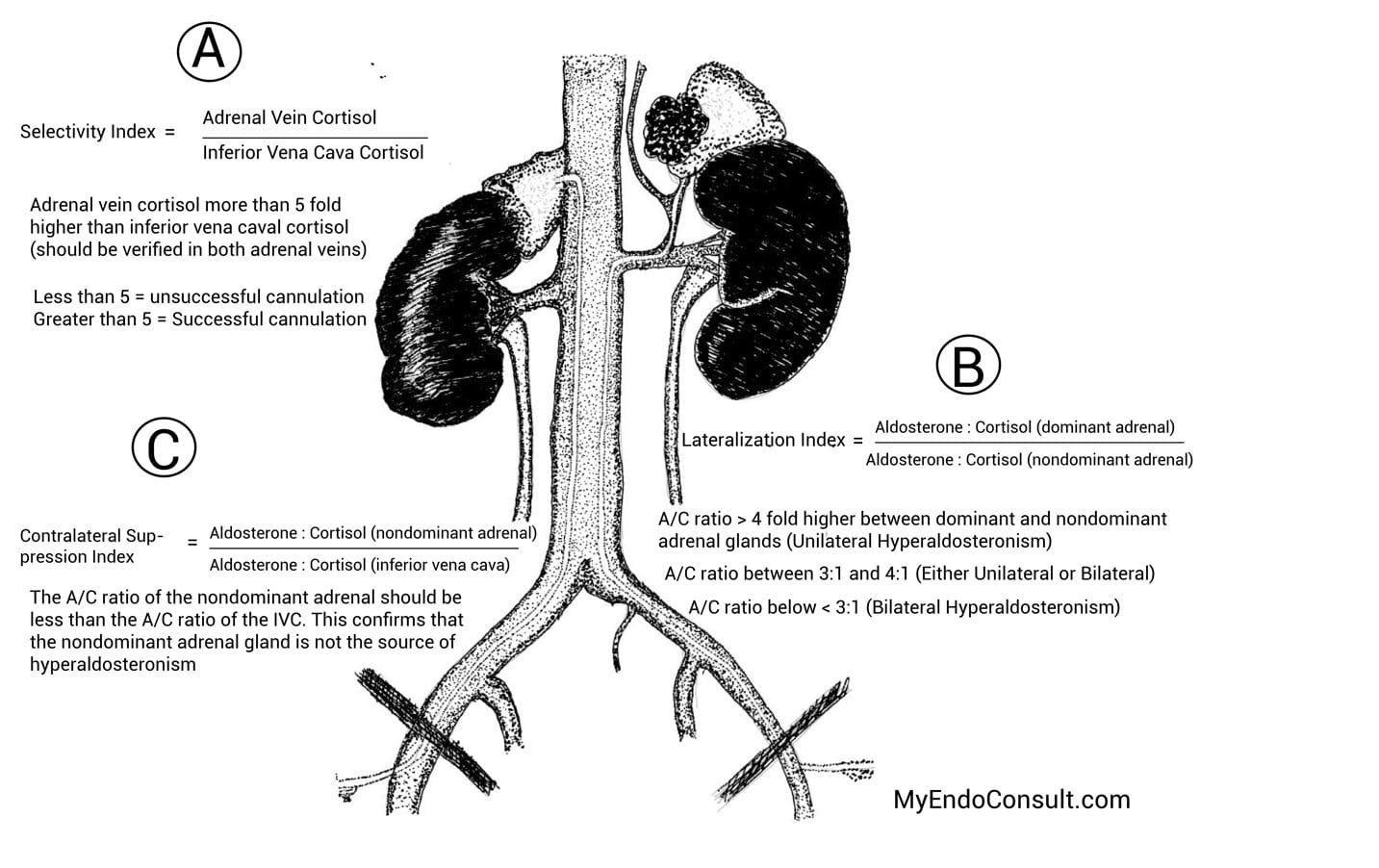
PRIMARY ALDOSTERONISM (PA) Definition and Subtypes Primary Aldosteronism (PA) : Characterized by hypertension, suppressed renin, and increased aldosterone secretion (Conn, 1955).Main Subtypes :Bilateral Idiopathic Hyperaldosteronism (IHA) : Most common.Aldosterone-Producing Adenoma (APA) : Also common.Unilateral Adrenal Hyperplasia (UAH) : Rare, unilateral zona glomerulosa hyperplasia.Familial Hyperaldosteronism (FH) :Type I (Glucocorticoid-Remediable Aldosteronism, GRA) : Autosomal dominant, suppressed by exogenous glucocorticoids.Type II : Familial occurrence of APA and/or IHA.Ectopic Aldosterone Secretion (very rare, e.g., ovarian tumor).Clinical Presentation Prevalence : ~5% of all hypertension cases (most common identifiable secondary HTN).Many Patients : Normal serum potassium (no hypokalemia).Hypokalemia (if present) : May cause alkalosis, nocturia, polyuria, muscle cramps, palpitations, positive Chvostek/Trousseau signs .Suspect PA :Hypertension + Hypokalemia. Resistant (treatment-refractory) hypertension. Hypertension + Adrenal incidentaloma. Onset of hypertension <20 years old. Severe hypertension. Case-Finding and Confirmation Screening Test : Morning (8–10 am) ratio of Plasma Aldosterone Concentration (PAC) to Plasma Renin Activity (PRA) .Avoid MR antagonists or high-dose amiloride. Correct hypokalemia first to avoid false negatives. PAC:PRA ratio has ~75% sensitivity/specificity. Elevated ratio → proceed to confirmatory aldosterone-suppression testing (oral sodium loading, saline infusion, captopril test, or fludrocortisone test). Subtyping Imaging (CT) of adrenals is done, but non-diagnostic in many cases.Adrenal Venous Sampling (AVS)Treatment Options Unilateral Aldosterone Excess (APA or UAH): Unilateral laparoscopic adrenalectomy → corrects hypokalemia, improves HTN (30–60% cured).Bilateral Idiopathic Hyperaldosteronism (IHA) or Familial Hyperaldosteronism Type I (GRA) :Medical therapy with Mineralocorticoid Receptor (MR) antagonist (e.g., spironolactone, eplerenone).Goal : Not only lower BP but also block/minimize aldosterone’s harmful cardiovascular effects.THE BIOLOGIC ACTIONS OF ALDOSTERONE Regulation of Aldosterone Secretion Stimulators :Angiotensin II (RAAS)Hyperkalemia ACTH (minor)Inhibitors :Atrial Natriuretic Factor (ANF)Hypokalemia About 50–70% of aldosterone is bound (to albumin, CBG); 30–50% free. Half-life: ~15–20 min. Normal blood aldosterone: 0–21 ng/dL. Classic Roles Regulation of ECF Volume & Potassium Homeostasis .Binds mineralocorticoid receptor (MR) in distal nephron → promotes Na⁺ reabsorption in exchange for K⁺/H⁺ excretion. Angiotensin II → negative feedback loop with ECF volume.MR Tissue Distribution : Highest in kidney (distal tubule), colon, hippocampus. Lower in heart, GI tract, etc.Mechanism : Increases expression of aldosterone-regulated kinase → modifies apical Na⁺ channels → ↑Na⁺ reabsorption → negative luminal charge → ↑K⁺ & H⁺ excretion.Intracellular processes (mechanism of action of aldosterone) Mineralocorticoid Escape After 3–5 days of high mineralocorticoid exposure, escape phenomenon occurs: various counterregulatory mechanisms (renal hemodynamics, ANP, etc.) limit continued volume expansion. Nonclassic Effects Nongenomic Actions : Rapid cell surface receptor (likely G protein–coupled) modifies sodium-hydrogen exchange.Tissue Fibrosis and Injury : Aldosterone can induce collagen gene expression, TGF-β, PAI-1 → possible microangiopathy, fibrosis in heart, vessels, kidney. Imbalance between volume state & aldosterone is key.ADRENAL VENOUS SAMPLING (AVS) FOR PRIMARY ALDOSTERONISM Rationale Distinguish unilateral aldosterone-producing adenoma (APA) vs. bilateral hyperaldosteronism (IHA).Imaging (CT) is only ~50% accurate. AVS is gold standard for subtyping if surgical cure is pursued.Protocol Patient Preparation Control BP but hold MR antagonists (spironolactone) a few weeks prior. Some centers use continuous cosyntropin (ACTH) infusion to stabilize aldosterone secretion. Procedure Femoral vein approach → selective catheterization of both adrenal veins + a reference vein (IVC or external iliac). Radiographic contrast to confirm correct catheter tip position. Blood sampling for aldosterone & cortisol from each adrenal vein + reference site. Interpretation Cortisol levels confirm correct catheterization. Compare aldosterone/cortisol ratios from each side to reference. Unilateral disease: Markedly elevated ratio on one side, suppressed on contralateral.Bilateral disease: Similar ratios both sides.Complications ~2.5% rate in experienced centers: groin hematoma, adrenal hemorrhage, vein dissection. Interpretation of AVS RENIN–ANGIOTENSIN–ALDOSTERONE SYSTEM (RAAS) AND RENOVASCULAR HYPERTENSION RAAS Basics Renin :Produced by juxtaglomerular cells in kidney. Rate-limiting step converting angiotensinogen → angiotensin I. Stimulated by low renal perfusion, low tubule NaCl (macula densa), sympathetic tone. Suppressed by high BP, high sodium, etc. Angiotensin I → II Via angiotensin-converting enzyme (ACE) . Angiotensin II → vasoconstriction, aldosterone secretion, increased sympathetic outflow, vasopressin release, etc. Aldosterone Final effector in Na⁺ reabsorption, K⁺ excretion. ECF volume & BP regulation. RAAS Pathway Renovascular Hypertension Cause : Renal artery stenosis (atherosclerosis or fibromuscular dysplasia) → decreased perfusion → ↑renin → ↑angiotensin II → ↑aldosterone → HTN.Suspicion :Onset <30 years or >55 years with no risk factors/family history. Sudden severe or treatment-resistant HTN. Unexplained atrophic kidney, rise in creatinine after ACE inhibitor, etc. Diagnosis :Gold standard: Renal arteriography . Less invasive: MR angiography , CT angiography , Duplex Doppler US . Post navigation