The meaning of the fairly simple T3 resin uptake test (also known as the Resin T3 uptake test, RT3U) is commonly misunderstood. Because of its name, many doctors think it measures the concentration of T3, which in fact, it does not. In this article, we will review the steps in performing this test, pathophysiologic principles underlying the test and some cases studies.
How is the Resin T3 Uptake test performed?
The test consists of adding triiodothyronine (T3) labeled with radioactive iodine (either 125-I or 131-I isotopes) to the patient’s serum. After a short incubation, radioactive iodine labeled T3 binds in part to the available hormone-binding sites of the binding proteins (mainly thyroxine-binding globulin).
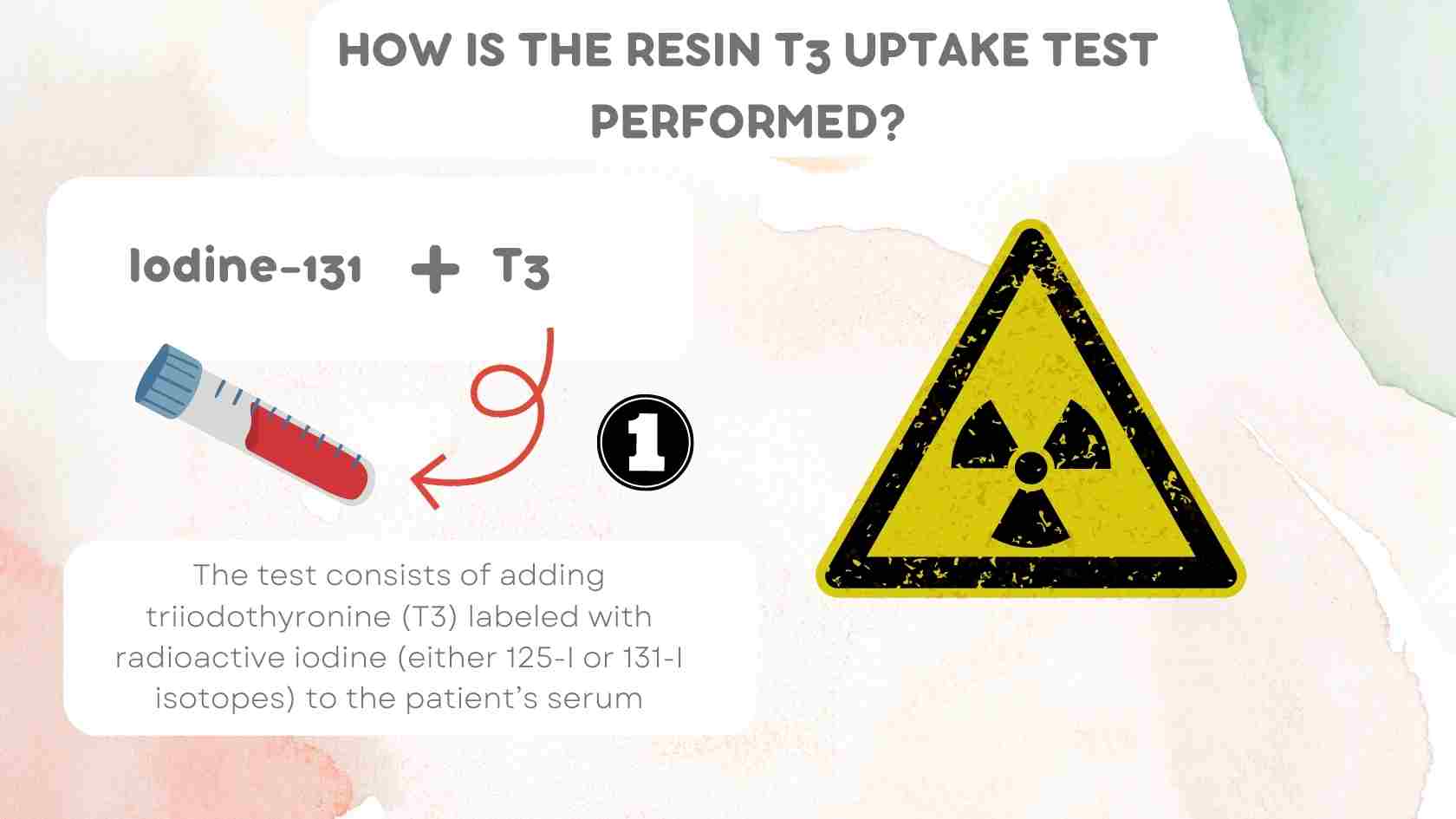 Triiodothyronine (T3) labeled with radioactive iodine (I-131 isotope) to the patient’s serum
Triiodothyronine (T3) labeled with radioactive iodine (I-131 isotope) to the patient’s serum
The free (unbound) radiolabeled hormone is absorbed onto an anion-exchange resin, and the radioactivity on the resin is measured (hence the name “Resin T3 uptake”)
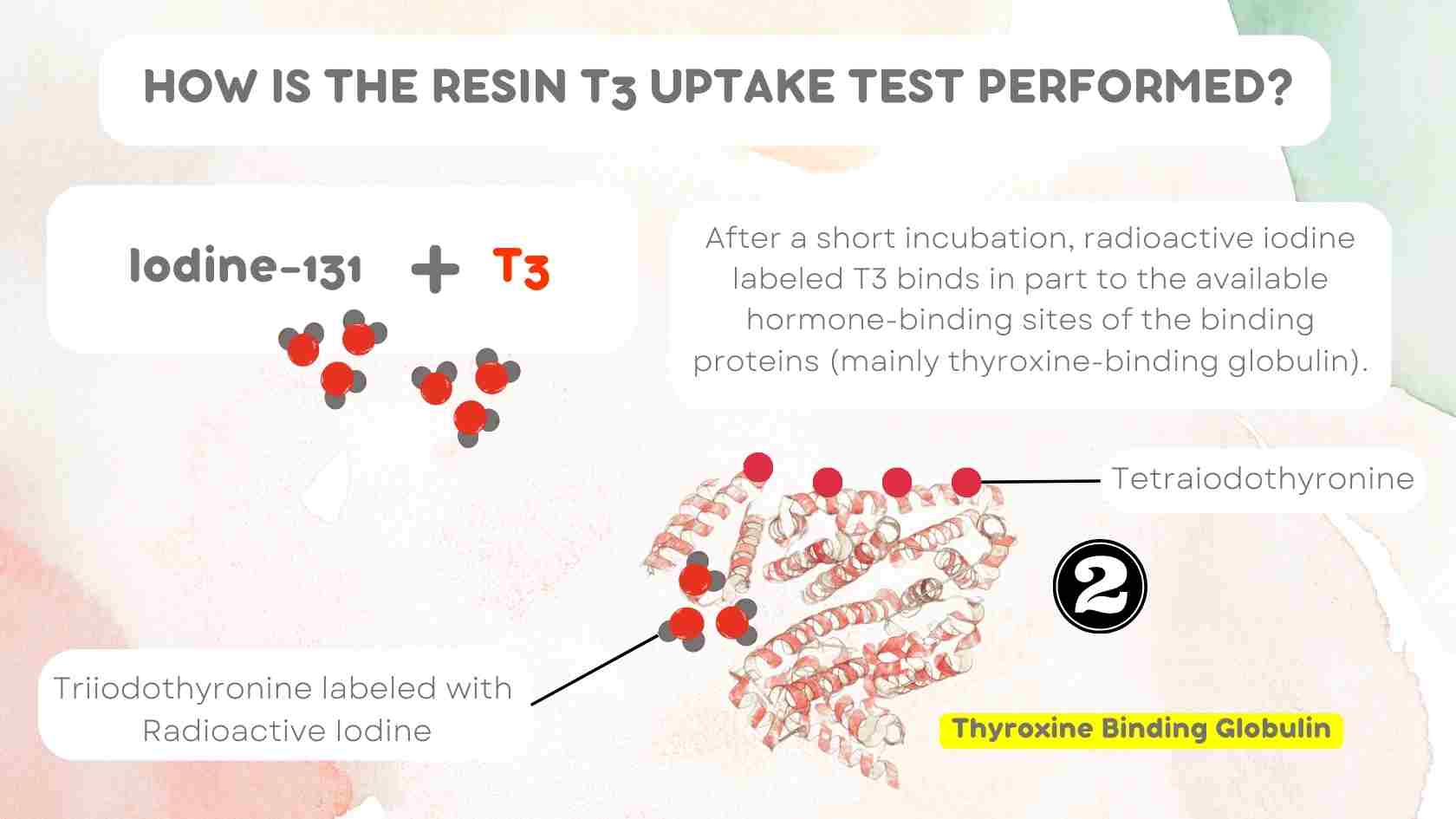 Radioactive iodine labeled T3 binds in part to the available hormone-binding sites
Radioactive iodine labeled T3 binds in part to the available hormone-binding sites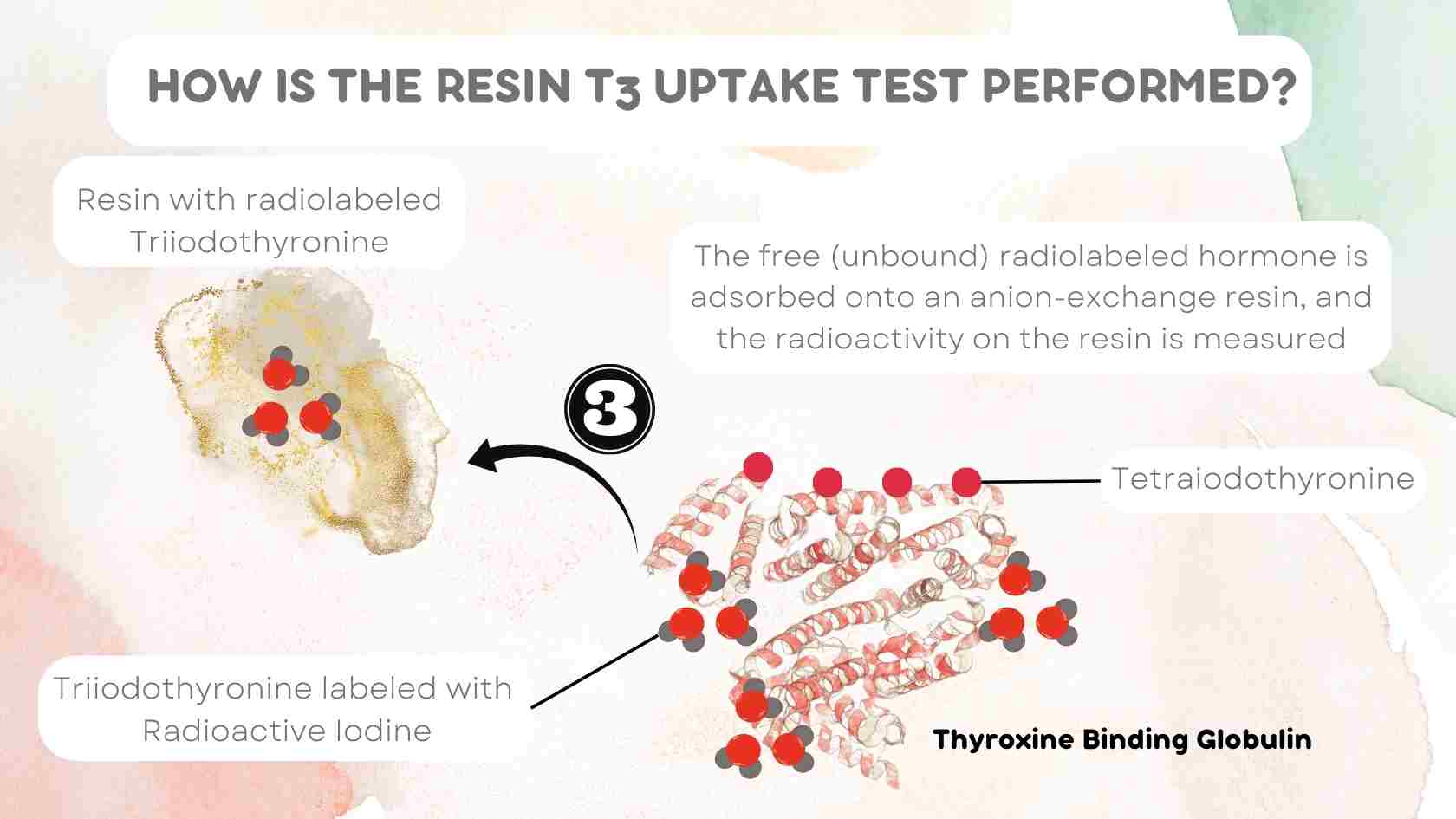 Free (or unbound) radioactive iodine labeled T3 is then absorbed onto an anion-exchange resin
Free (or unbound) radioactive iodine labeled T3 is then absorbed onto an anion-exchange resin
Interpretation of the T3RU test
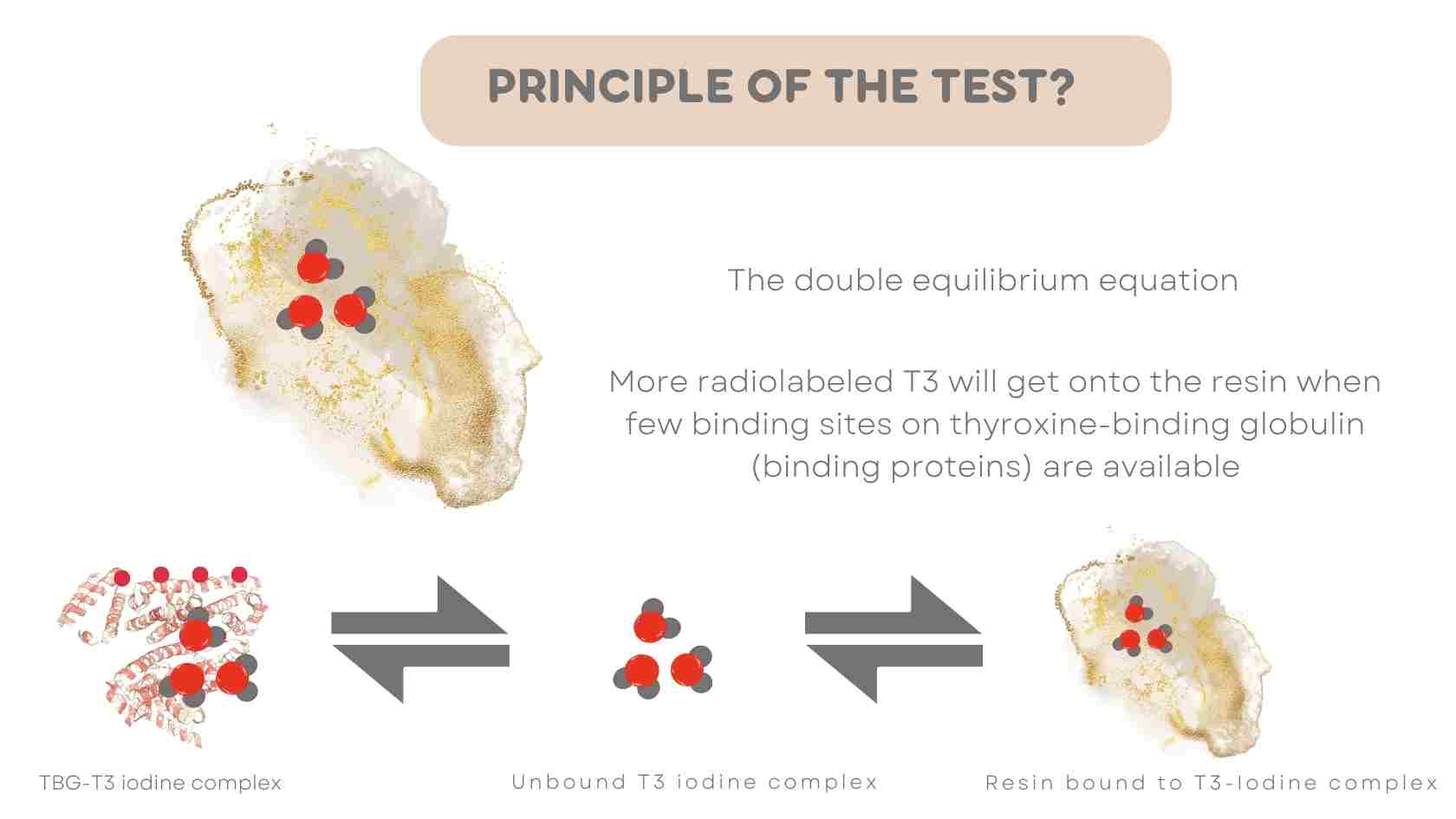
Next, we will review the interpretation of this test. In order to understand how to interpret the test, we must first review the double equilibrium equation for the T3 resin uptake test.
This equation shows that radioiodine labeled T3 bound to binding proteins in the serum is in equilibrium with unbound radioiodine labeled T3 and bound radioiodine labeled T3 (which is the portion attached to the resin).
For a patient without underlying thyroid dysfunction, about 25 % to 35 % of the added radioiodine labeled T3 goes onto the resin.
 Double Equilibrium Equation for T3 Resin Uptake
Double Equilibrium Equation for T3 Resin Uptake
Equilibrium EquationBinding Protein-T3 131-I complex = free T3 131-I = Resin bound T3 131-I
Inspection of the double equilibrium above shows that more radioactivity will go onto the resin when few binding sites on thyroxine-binding globulin (binding proteins) are available.
This is the case in hyperthyroidism since the excess thyroid hormone occupies binding sites on thyroxine-binding globulin that are normally free.
A decrease in free binding sites, and therefore a high T3 resin uptake, also occurs when the amount of binding protein in plasma is diminished or when the binding sites are occupied by a drug such as salicylate.
Now let us assess our understanding of this test in another case scenario. What will be the expected T3 resin uptake in a patient with hypothyroidism?
In hypothyroidism, due to a decrease in the serum thyroxine concentration, many binding sites on thyroxine-binding globulin are free. A larger fraction of the radiolabeled T (T3 131-I) will be bound to the protein, and correspondingly less to the resin, i.e., the resin T3 uptake is low.
Conceptually, the same result will also be obtained in cases where the overall number of available binding sites is increased, as would be expected in the setting of increased concentration of thyroxine-binding globulin.
This is the case in estrogen or oral contraceptive treatment and also during pregnancy. This is because of estrogen-mediated increased production and decreased clearance of thyroxine-binding globulin (due to sialylation).
What is Sialylation:Increased sialic acid content of the TBG molecule
The resin T3 uptake (or T3 resin uptake) thus has a direct relationship to the serum concentration of thyroxine and an inverse relationship to the concentration of hormone-binding protein (thyroxine-binding globulin).
By itself, the T3 resin uptake test is not a very sensitive test for thyroxine concentration, and it should, therefore, never be performed alone.
Indeed, it should always be combined with the measurement of T4 in serum. The advantage of the test lies in the fact that it allows the detection of the relatively frequent states with altered hormone- binding protein concentration. If the results of the two tests are compatible, the binding proteins of plasma are normal.
If, in contrast, one test indicates hypothyroidism and the other hyperthyroidism, there has been some change in the binding proteins (that is, thyroxine binding globulin). The various possibilities are explained in detail in the table below.
Mechanism of T3 Resin Uptake Test
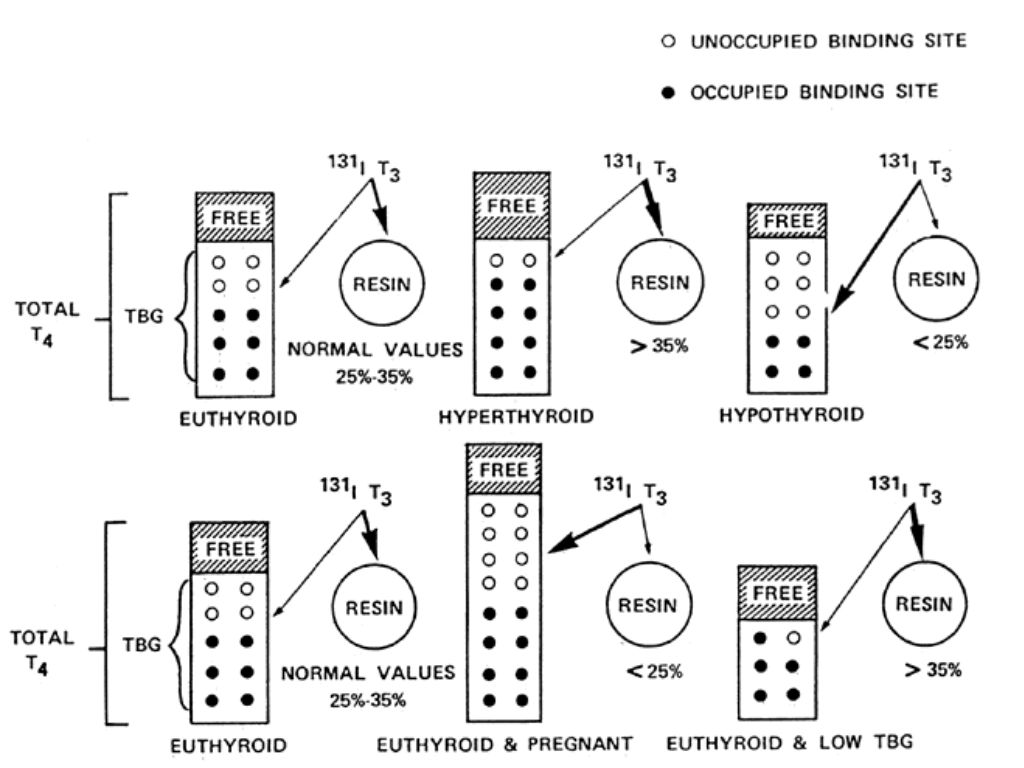 Fig.1 Schematic representation of the mechanisms underlying RT3U in various endocrine states. Mestman JH: Thyroid and parathyroid diseases. In Quilligan EJ, Kretchmer N [eds]: Fetal and Maternal Medicine, p 493. New York, John Wiley & Sons, 1980
Fig.1 Schematic representation of the mechanisms underlying RT3U in various endocrine states. Mestman JH: Thyroid and parathyroid diseases. In Quilligan EJ, Kretchmer N [eds]: Fetal and Maternal Medicine, p 493. New York, John Wiley & Sons, 1980
Table 1. Comparison of Total T4 and RT3U in various thyroid states
| Thyroid State | Total T4 | RT3U (25 % to 35 %) |
| Euthyroidism, Normal TBG (normal binding proteins) | Normal | Normal |
| Euthyroidism, high TBG (estrogen-mediated) | High | Less than 25% |
| Euthyroidism, low TBG (nephrotic syndrome, chronic liver disease, inherited defect) | Low | Greater than 35% |
| Hyperthyroidism, normal TBG | High | Greater than 35% |
| Hypothyroidism, normal TBG | Low | Less than 25% |
Table 2. Causes of low and high RT3U
| High RT3U | Low RT3U |
| Hyperthyroidism | Hypothyroidism |
| Low protein states (cirrhosis, nephrotic syndrome, protein losing enteropathy) | Pregnancy |
| Congenital X-linked deficiency in TBG. | Congenital X-linked TBG Excess states |
| Cushing’s Disease | Hepatitis |
| Acromegaly | Porphyria |
| Medications (androgens, salicylates, anabolic steroids and glucocorticoids) | Medications (estrogen, oral contraceptive pills, clofibrate) |
Free Thyroxine Index
As discussed previously, the combined evaluation of the Total T4 concentration and the RT3U allows a correct diagnosis of thyroid function even in the setting of expected variations in hormone-binding proteins of plasma.
The combined tests thus give us a better idea of the concentration of the functionally relevant free thyroid hormone. The free Thyroxine Index is assessed quantitatively by multiplying the Total T4 concentration by the estimated RT3U.
The thyroxine-resin T3 index (also known as the Free Thyroxine Index) thus obtained is an abstract number that correlates very closely with the free hormone concentration.
FTI = Total T4 of the patient x (T3RU patient / T3RU mean control)
The Free T4 index is expressed without units.
T3RU in the control group is assessed by calculating the mid-normal T3RU for samples evaluated at the laboratory performing the test.
Conclusion
The free thyroxine index was relevant at a time when the direct assessment of free T4 was labor-intensive and cumbersome. Since the discovery of high throughput radioimmunoassays (RIA) for the assessment of hormones, free T4 evaluation is easy in routine practice.
Consequently, thyroid function tests such as the Free Thyroxine Index and RT3U are discussed due to their historical importance.
I hope you found this article helpful.