Skip to content January 11, 2025
Thyroid Carcinomas Home › 9 min read
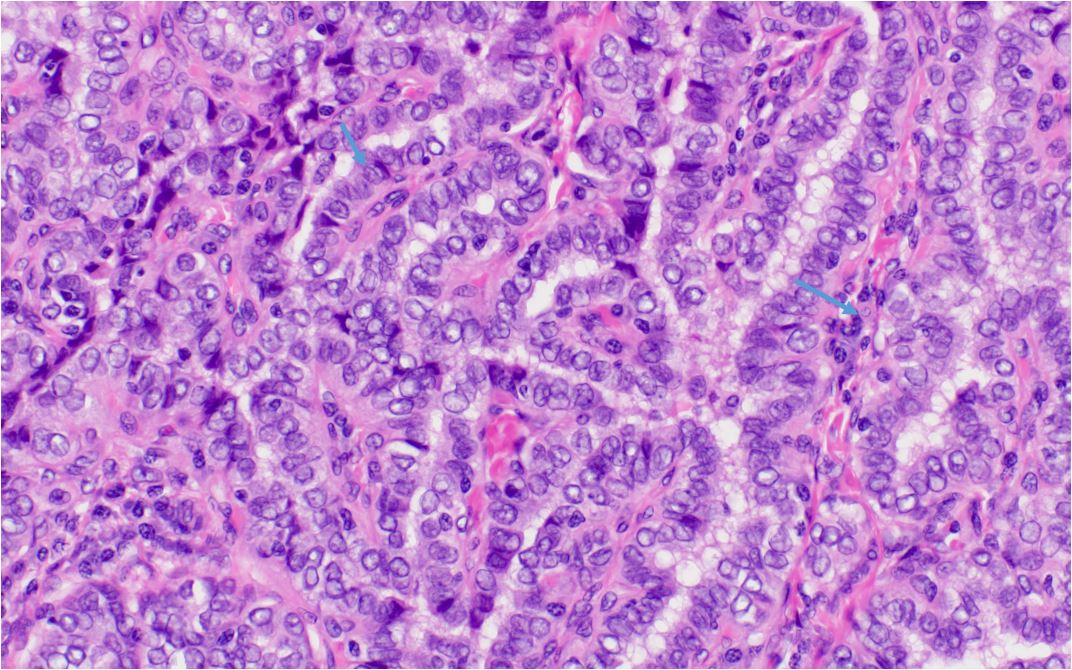
PAPILLARY THYROID CARCINOMA (PTC) Definition and Prevalence Papillary Thyroid Carcinoma (PTC) : One of three thyroid epithelial–derived carcinomas (the others are follicular and anaplastic).Most common malignant thyroid tumor : ~75% of thyroid cancer cases.Peak Incidence : 4th and 5th decades of life (i.e., ages 30s to 50s).Gender Predominance : ~2.5:1 ratio in women vs. men.Clinical Presentation Thyroid Nodule Often presents as a solitary thyroid nodule . Increasingly detected incidentally on imaging (CT, ultrasound) done for other reasons. Multifocality PTC frequently has multiple foci within the thyroid. When presenting via cervical lymph node biopsy showing “papillary lesion,” at least half of the intrathyroidal foci may be genetically distinct (independent clones). Histopathology Gross and Microscopic Features Typically unencapsulated . Characterized by papillary cords with delicate vascularized stroma lined by cuboidal/columnar cells. Pure PTC usually lacks colloid/follicles.Nuclear Features :Large, oval nuclei with hypodense (Orphan Annie–eye) chromatin . Cytoplasmic “pseudoinclusions” (redundant nuclear membrane). Psammoma Bodies : Found in ~50% of PTC (calcified, scarred remains of tumor papillae).Papillary thyroid carcinoma, classic nuclear features
Marked nuclear enlargement (compare to normal thyroid follicular epithelium)
Nuclear crowding
Grooves (short arrow)
Nuclear condensation to the periphery of the nucleus (Orphan Annie Eye)
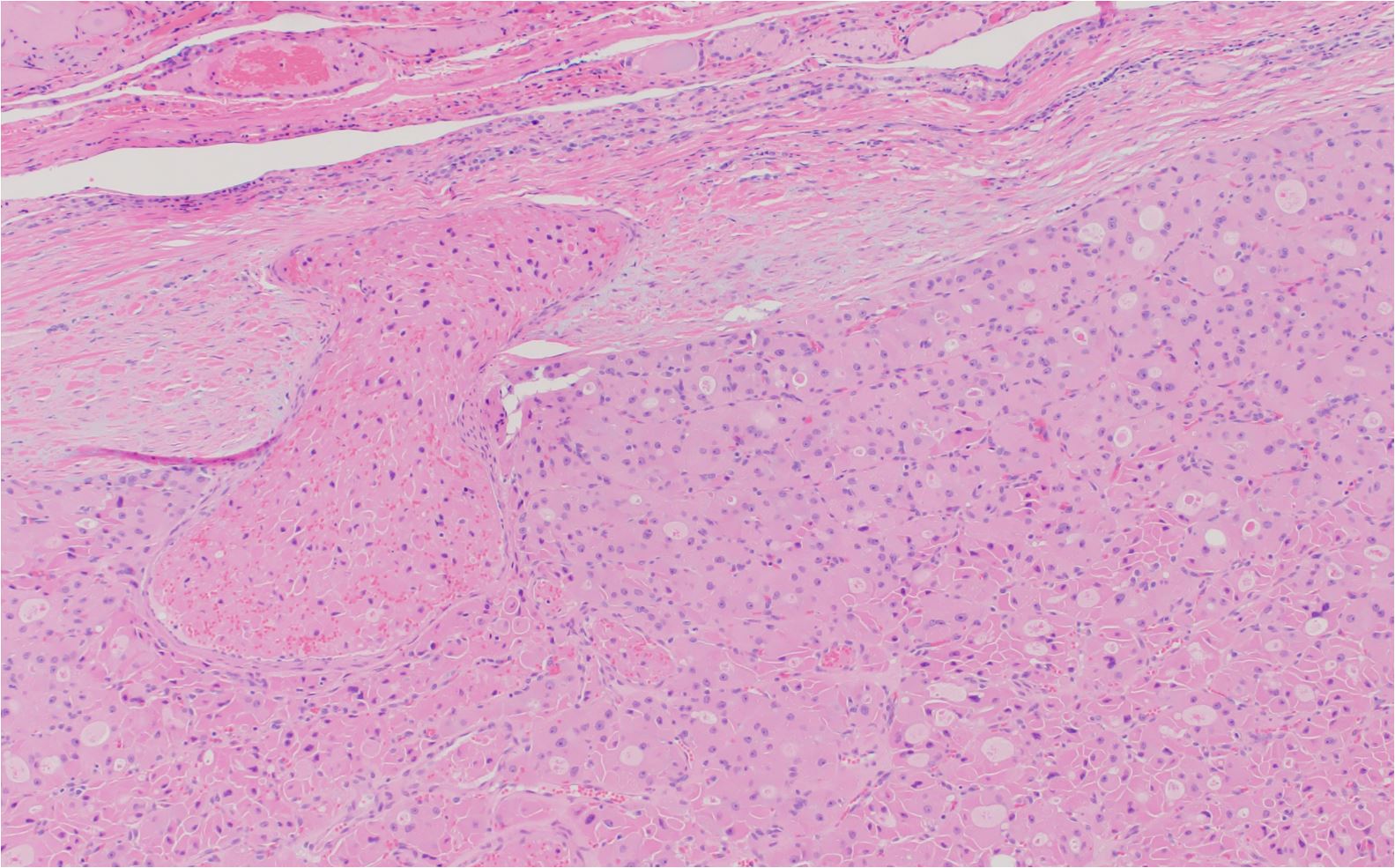
Papillary architecture characterized by fibrovascular core (long arrow) Variants Follicular Variant (~10%): Follicles plus classic PTC nuclear changes; overall prognosis similar to classic PTC.Tall-Cell Variant (~1%): More aggressive; larger, more invasive.Other Rare Variants (e.g., clear-cell, insular, columnar, trabecular, oxyphilic, diffuse sclerosing) → often more aggressive behavior.Metastatic Patterns Regional Lymph Nodes (cervical, upper mediastinal) frequently involved.Distant Metastases are uncommon at initial diagnosis (~2%):Lung is the most frequent distant site (often showing miliary pattern on imaging).Bone less common (more likely in older patients).Rare sites: Brain, liver, kidney, adrenal glands. Staging of Thyroid Carcinoma Prognosis and Risk Factors Overall Behavior One of the least aggressive human cancers; many patients do not die of PTC. Still can be fatal in some cases, especially if high-risk features present. High-Risk Features for Recurrence/Mortality Age >45 years at diagnosis. Tumor size >7 cm. Soft-tissue invasion (e.g., trachea, esophagus). Additional risk factors: Male gender, multicentric PTC, >10 lymph node metastases, age <7 years. Treatment Surgical Management Total Thyroidectomy + Central Compartment Lymphadenectomy for PTC >1 cm or with known nodal metastases.More extensive surgery if there is extrathyroidal invasion (trachea, esophagus). Less Extensive Resection (lobectomy + isthmusectomy) may suffice for solitary PTC <1 cm.Radioactive Iodine (131I)Adjuvant therapy to ablate residual microscopic disease. Not universally used; patient selection is individualized. External-Beam Radiotherapy Considered in unresectable disease not responsive to 131I. Chemotherapy / Targeted Therapy Systemic chemotherapy for aggressive, symptomatic, refractory disease.Tyrosine Kinase Inhibitors and other molecular pathway–blocking drugs under investigation for refractory cases.Thyroid Hormone SuppressionLevothyroxine therapy postoperatively to suppress TSH and reduce tumor stimulation.FOLLICULAR THYROID CARCINOMA (FTC) Definition and Incidence One of three thyroid epithelial–derived cancers (others: papillary carcinoma, anaplastic carcinoma).Second most common thyroid cancer after papillary thyroid carcinoma (PTC), accounting for ∼10% of all thyroid malignancies.Demographics and Risk Factors Peak Incidence : 40–60 years of age.Female : Male ratio ~3:1.Geographic Iodine Deficiency : More common in iodine-deficient regions.Clinical Presentation Thyroid Nodule or Mass May be small or large. Typically solitary intrathyroidal focus (unlike PTC, which can be multifocal). Fine-Needle Aspiration (FNA) Limitations Cytology cannot distinguish FTC from a benign follicular adenoma . Definitive diagnosis requires histologic evidence of tumor capsule or vascular invasion from en bloc surgical specimen. Histopathology Follicular Pattern Organized follicles lined by high cuboidal epithelium, often containing colloid. No papillary features (e.g., no psammoma bodies).Capsular or Vascular Invasion Hallmark for malignancy (distinguishes from benign adenoma). Subtypes Minimally Invasive FTC : Encapsulated, better prognosis.Widely Invasive FTC : Invades blood vessels and adjacent thyroid tissue; worse prognosis.Molecular Genetics Often monoclonal ; ~40% have RAS point mutations, associated with more aggressive behavior. Metastasis and Spread Hematogenous Dissemination : Common; distant metastases in ~15% of patients at diagnosis.Most Frequent Sites : Bone, lung (less commonly liver, brain, urinary bladder, skin).Lymph Node Metastases : Much less common than in PTC.Skeletal Metastases : May histologically resemble normal thyroid tissue.Prognosis Generally More Aggressive than papillary carcinoma.Poor prognosis factors:Larger Tumors Distant Metastasis Vascular Invasion Insular Carcinoma : A poorly differentiated FTC variant with a poor prognosis.Hürthle Cell Carcinoma Hurthle cell carcinoma with a focus of vascular invasion into a thick capsule Treatment Surgical Management Total Thyroidectomy + Central Neck Lymph Node Dissection = standard of care.Preoperative neck ultrasonography for lymph node mapping is essential. Radioactive Iodine (131I)FTC cells can take up 131I but less efficiently than normal follicular cells. 131I used post-thyroidectomy to ablate remnant thyroid and microscopic metastatic disease. Thyroid Hormone SuppressionLevothyroxine replacement post-surgery to suppress TSH, aiming to prevent TSH-driven tumor growth.External-Beam Radiation Therapy Used if residual primary or metastatic disease is unresectable. Chemotherapy and Targeted Therapy Systemic chemotherapy for disease refractory to other treatments. Molecular pathway inhibitors (e.g., tyrosine kinase inhibitors) under investigation for refractory cases.MEDULLARY THYROID CARCINOMA (MTC) Definition and Incidence Neoplasm of Thyroid “C Cells” : Parafollicular cells derived from the embryonic neural crest.Accounts for ~3% of all thyroid malignancies.More accurately considered a neuroendocrine tumor rather than a conventional thyroid carcinoma. Sporadic vs. Familial Sporadic MTC ~80% of cases. Typically presents as a solitary thyroid nodule in patients aged 40–60 years ; slight female preponderance. At diagnosis, >50% have regional lymph node metastases . Familial MTC Associated with MEN 2A , MEN 2B , or Familial MTC (FMTC) . Inherited in an autosomal dominant fashion with RET proto-oncogene mutations . Penetrance ~100% in MEN 2 syndromes.MEN 2B form is more aggressive; prophylactic thyroidectomy is recommended in the first year of life .Clinical Features and Metabolism Calcitonin Secretion : Elevated serum calcitonin can cause severe diarrhea .May secrete other hormones (e.g., ACTH → Cushing syndrome ). Fine-Needle Aspiration (FNA) typically diagnostic in solitary thyroid nodule.Histopathology Solid Trabecular Pattern Closely packed cells with variable nuclear size/hyperchromatism. Immunostaining Calcitonin , Galectin-3 , Carcinoembryonic Antigen (CEA) .Genetic Testing RET Proto-Oncogene All patients with MTC should have genetic testing because ~7% of apparently sporadic cases harbor a RET mutation. Identifies at-risk family members; allows early (prophylactic) thyroidectomy to prevent metastases. Coexisting Endocrine Disorders Management Surgical Treatment Total Thyroidectomy is the treatment of choice.Prognosis correlates with age at diagnosis ; familial cases have better outcomes if operated on earlier. Monitoring Serum Calcitonin postoperatively to assess for surgical cure.Persistent elevated calcitonin suggests residual or metastatic disease. Advanced Disease Metastases may involve neck nodes , mediastinum , lungs , liver , bone , kidneys . Molecular pathway–blocking drugs (e.g., tyrosine kinase inhibitors) for unresectable or refractory disease.HÜRTHLE CELL THYROID CARCINOMA (HCC) Definition and Incidence Variant of Follicular Thyroid Carcinoma (FTC), also called the oncocytic variant of FTC.Accounts for 3%–4% of all thyroid malignancies. Distinctive Oncocytes (Hürthle or oxyphilic cells) constitute ≥75% of the tumor.Demographics Age Range : Peak incidence at 40–70 years , median ~61 years.Gender : Approximately 2:1 female to male ratio.Typically presents as a painless solitary thyroid nodule , which may vary in size. Pathology and Histology Gross Appearance Often mahogany-brown tumor(s) on gross examination. Microscopic Features Oncocytes : Eosinophilic, oxyphilic cells with abundant granular cytoplasm (packed with mitochondria).Cells arranged in trabecular or plexiform patterns, separated by a dense capillary network. Scant or No Colloid present.Nuclei : Hyperchromatic, pleomorphic, prominent eosinophilic nucleoli.Carcinoma Diagnosis depends on capsular invasion , vascular invasion , or metastasis .Radioiodine Uptake <10% of HCC lesions show significant radioiodine uptake . Clinical Behavior and Metastasis Comparative Aggression More aggressive than standard follicular or papillary thyroid carcinoma. Metastases ~5% have distant metastases (lung or bone) at diagnosis. ~25% have regional lymph node metastases. Prognostic Factors Distant Metastases at presentation → strong predictor of poor outcome.Older Age , Larger Tumor Size , Male Gender , Extrathyroidal Invasion → worsen prognosis.Recurrence Rate ~35% overall recurrence post-surgery. Treatment and Management Surgical Approach Total Thyroidectomy + Ipsilateral Central Neck Lymph Node Dissection (similar to FTC).Adjuvant Therapy Radioiodine typically not beneficial (low uptake).External-Beam Radiotherapy may be considered for unresectable disease.Systemic or Targeted Therapy Molecular pathway–blocking drugs (e.g., tyrosine kinase inhibitors) may help in refractory cases.ANAPLASTIC THYROID CARCINOMA (ATC) Definition and Incidence Undifferentiated Thyroid Cancer : One of three epithelial-derived thyroid cancers (alongside papillary and follicular).Rare but Highly Malignant : ~2% of all thyroid malignancies.Demographics :Typically occurs after age 50 (mean ~65 years). ~Two-thirds of cases occur in women . Clinical Presentation Rapid Neck Mass Growth Patients often recall a precise recent onset and describe rapid enlargement. Usually painful/tender with local pressure symptoms (dyspnea, dysphagia, hoarseness, cough). Systemic Symptoms Weight loss, anorexia, fatigue, fever. Physical Examination Large tumor (often >5 cm), hard, frequently fixed to surrounding tissues.Overlying skin may be warm or erythematous. Cervical adenopathy often present.Tracheal deviation, vocal cord paralysis (recurrent laryngeal nerve involvement). Possible superior vena cava syndrome if tumor compresses thoracic inlet. Pathogenesis and Precursor Lesions Association with Differentiated Thyroid Carcinoma :~20% have a history of PTC or FTC. ~50% have a history of goiter . Likely “Dedifferentiation” from existing neoplasm (loss of tumor suppressor or new activating mutation).Diagnosis Biopsy Fine-Needle Aspiration or surgical biopsy.Histology: Solid, highly anaplastic growth with spindle cells and giant cells. Imaging CT of neck/chest aids in evaluating tumor extent, tracheal compression, planning therapy.Metastasis and Local Invasion Local Invasion is rapid and lethal, infiltrating muscle, lymph nodes, trachea, esophagus, larynx, and major blood vessels.Cause of Death : Often tracheal compression/asphyxia.Distant Spread : Most commonly lungs , also bone, skin (chest wall), liver, heart, kidneys, adrenals.Prognosis and Treatment Surgery Complete resection if tumor is apparently confined to the thyroid, but recurrence within months is common. Adjuvant Therapy External-beam radiotherapy may be considered after surgery.Chemotherapy (e.g., paclitaxel) may provide brief partial responses.Survival Rarely exceeds 12 months from diagnosis. Essentially 100% disease-specific mortality .Post navigation