Skip to contentJanuary 11, 2025
Goiters
Home › 3 min read
EUTHYROID (NONTOXIC) GOITER
Definition and Overview
- Euthyroid (Nontoxic) Goiter: Enlargement of the thyroid gland without clinical signs of hyperthyroidism or hypothyroidism.
- Common in areas with low dietary iodine, but also seen elsewhere.
- Early stage often diffuse enlargement; later can become nodular (multinodular).
Clinical Presentation
- Age and Timing
- Often noted around puberty in both sexes when iodine intake is low.
- Gradual enlargement over many years, leading to various nodular patterns.
- Goiter Characteristics
- Diffuse Goiter initially; later may develop nodularity (hard areas, cystic areas).
- May be symmetric or asymmetric; can extend intrathoracically (substernal goiter).
- Obstructive Symptoms
- Tracheal Compression → dyspnea on exertion, stridor (in advanced cases).
- Esophageal Compression → dysphagia.
- Recurrent Laryngeal Nerve compression → vocal cord palsy.
- Cervical Sympathetic Chain compression → Horner syndrome.
- Pemberton Maneuver (raising arms) can elicit facial plethora, cyanosis, or stridor if thoracic inlet obstruction is present.
- Sudden Enlargement/Pain
- May be due to hemorrhage into a nodule or cyst.
- Pain can radiate to ear, shoulder, or neck structures.
- Possibility of Hyperfunction (“Hot Nodule”)
- Some nodules may become autonomously functioning → hyperthyroidism (toxic multinodular goiter).
- Cancer is rare but possible within a multinodular goiter.
Evaluation and Diagnosis
- Exclude Hyperthyroidism
- Measure serum thyrotropin (TSH).
- Thyroid Ultrasound
- Defines structure of nodules and extent of suprasternal goiter.
- CT/MRI
- Useful for substernal (intrathoracic) extension.
- Fine-Needle Aspiration Biopsy (FNA)
- If suspicious or prominent nodules are present to rule out malignancy.
Indications for Surgery
- Cosmetic Reasons
- Large, unsightly goiter size.
- Sudden Enlargement
- Rapid growth or a suspiciously hard area suggesting neoplastic change.
- Obstructive Symptoms
- Significant compression of trachea or esophagus, or thoracic inlet obstruction causing breathing/swallowing difficulties. (Review Pemberton Sign)
- Malignancy suggested by Fine Needle Biopsy
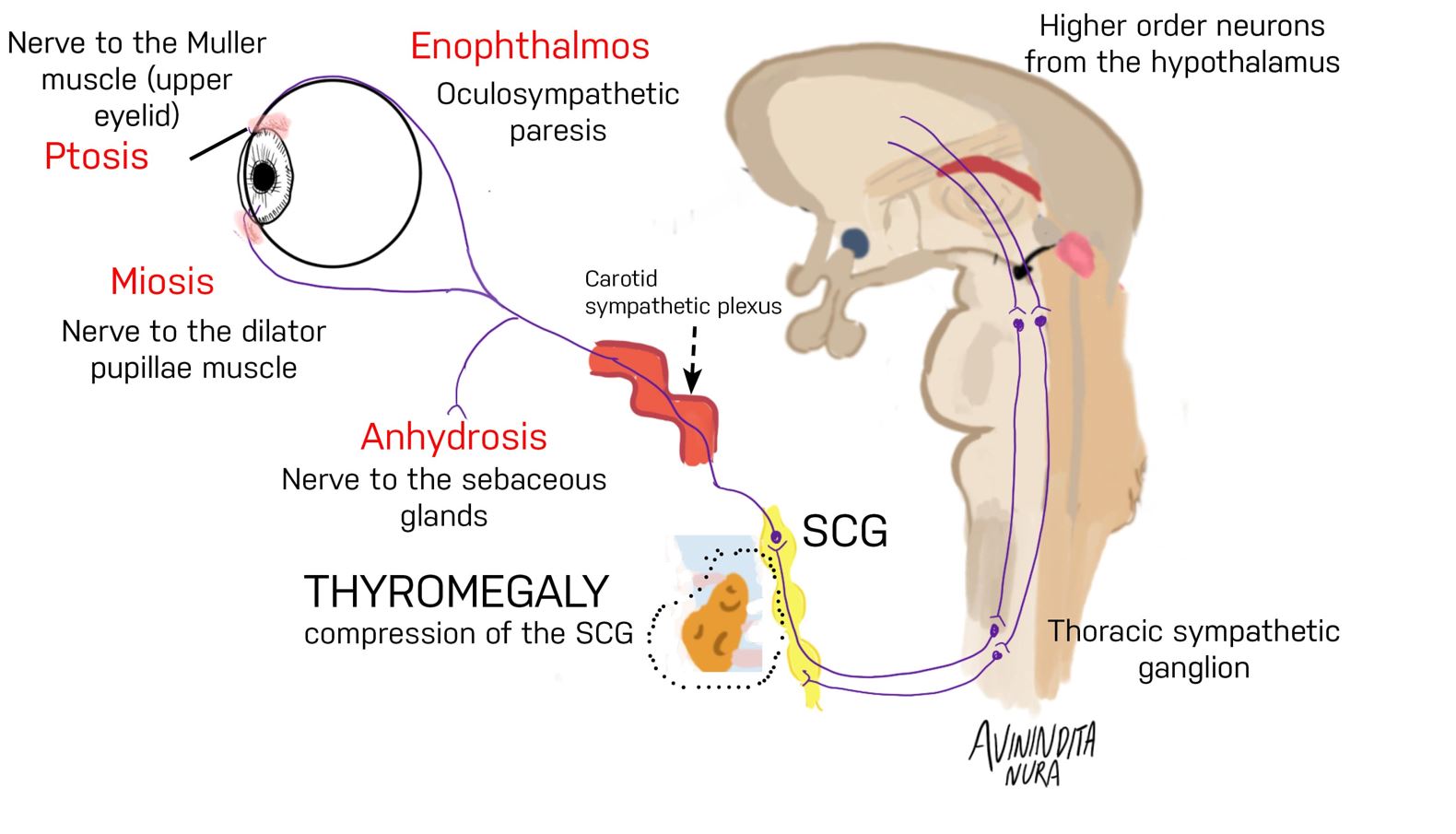 Horner’s syndrome on account of significant thyromegaly
Horner’s syndrome on account of significant thyromegaly
GROSS PATHOLOGY OF GOITER
Types and Frequency
- Goiter: Enlargement of thyroid, often related to dietary iodine intake.
- Nontoxic (Euthyroid) Goiters: Typically do not produce hypo- or hyperthyroidism, often appear during adolescence or pregnancy.
- Early Diffuse → eventually can become multinodular.
Physical Examination and Growth
- Gland can be 2–3× normal size or larger; patients may notice neck fullness, tight collars, difficulty swallowing.
- Compression of trachea → stridor; venous engorgement if thoracic inlet is narrowed.
- Gland feels firm (not hard). Over time, becomes asymmetric and nodular; nodules can differ in size and consistency.
Gross Appearance
- Large, nodular thyroid with possible hemorrhages, cysts, fibrosis, calcifications.
- Amber, translucent colloid on cut section.
- Some nodules are partially or fully encapsulated, mimicking follicular neoplasms.
- Rarely, cancer (e.g., papillary carcinoma) arises within a multinodular goiter.
Cytology and Histology
- Fine-Needle Aspiration from colloid nodules usually shows:
- Abundant colloid, mixed cell populations (follicular cells with uniform nuclei, inflammatory cells, Hürthle cells).
- Microscopy of multinodular goiter may show:
- Variable follicle size, some large (2 mm), coalescing into cystic areas.
- Rarely, malignant changes.
ETIOLOGY OF NONTOXIC GOITER
General Mechanism
- Often due to partial deficiency in thyroid hormone synthesis → increased TSH → thyroid hyperplasia/enlargement.
- Iodine Deficiency: Main environmental factor worldwide. About 1 billion people live in iodine-deficient regions.
- Dietary: The most important source of iodine (75 µg daily needed by thyroid; typical North American intake ~150–300 µg/day).
Inherited Defects (Dyshormonogenetic Goiters)
- Congenital enzyme defects in hormone synthesis (e.g., in NIS transporter, thyroglobulin, thyroid peroxidase, THOX2).
- Pendred Syndrome: Thyroid iodide transport defect + sensorineural deafness (pendrin protein abnormality).
- Thyroid Hormone Resistance: Mutations in thyroid receptor β can cause euthyroid goiter with elevated T4/T3.
Evolution of Nontoxic Goiter
- Early: Diffuse hyperplasia.
- Prolonged TSH Stimulation: Nodule formation, partial encapsulation, hemorrhage, cystic change, calcification.
- Involution: Epithelium flattens, colloid accumulates → large follicles and possible cysts.
- Rarely, carcinoma may arise.