Often discovered incidentally or when hypothyroid symptoms appear.
Clinical Course
Progression from subclinical to overt hypothyroidism over time (gradual loss of thyroid function).
Serologic Findings:
Elevated thyroid peroxidase (TPO) and thyroglobulin antibodies.
Primary hypothyroidism → elevated TSH.
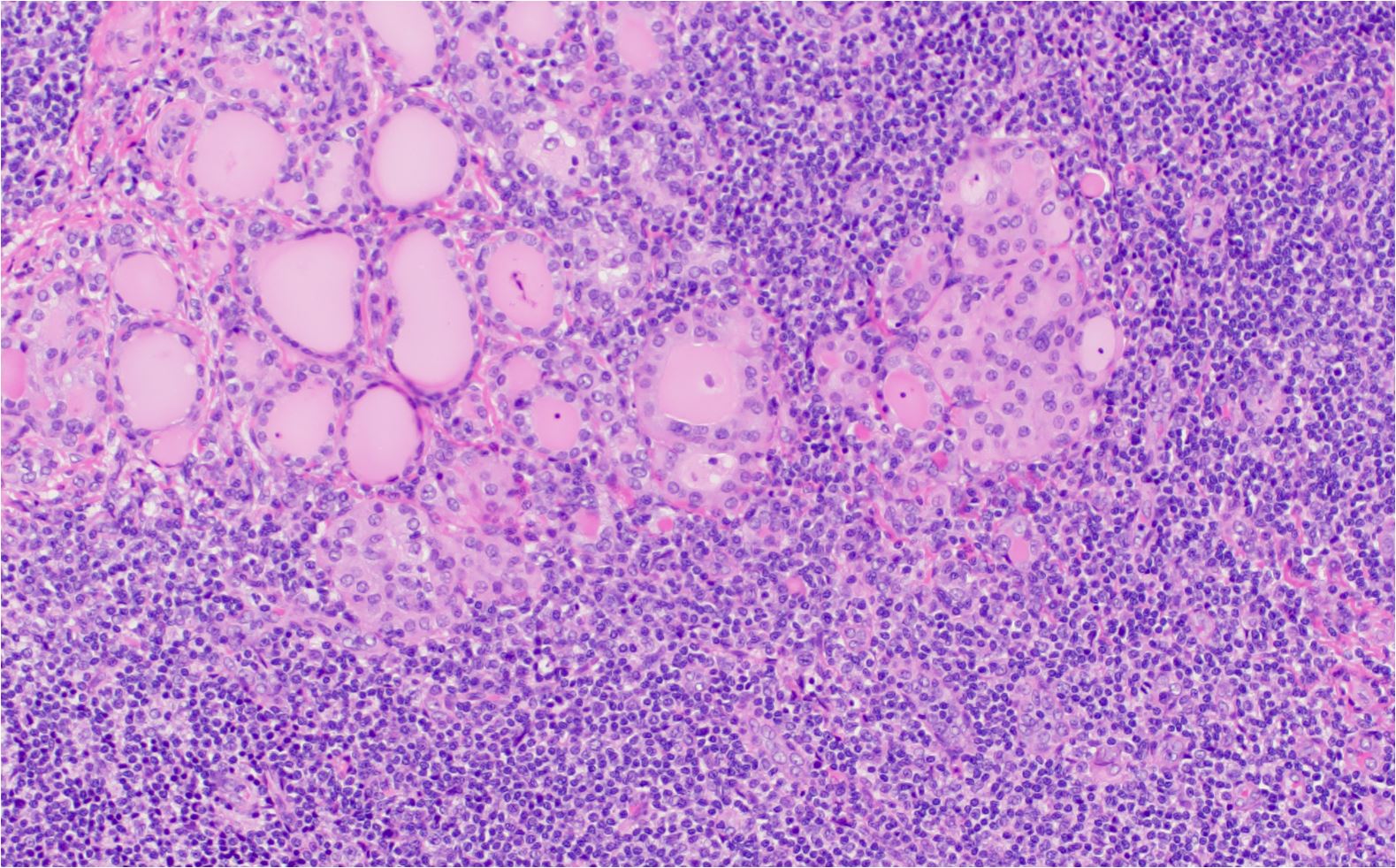
Hashimoto’s thyroiditis characterized by dense lymphoplasmacytic infiltrate and Hurthle cell metaplasia
Large areas of thyroid parenchyma are replaced by inflammatory infiltrate
Management
Levothyroxine replacement to correct hypothyroidism.
Thyroid biopsy usually unnecessary (diagnosis based on antibody tests + TSH).
Surgery only indicated for specific reasons, e.g., a large symptomatic goiter.
FIBROUS (RIEDEL) THYROIDITIS
Overview
Rare, primarily affects males.
Chronic proliferative fibrosing process involving the thyroid gland, potentially extending to trachea, esophagus, fasciae, muscles.
May be part of a systemic fibrosing disorder (e.g., also retroperitoneal or mediastinal fibrosis).
Pathology
Microscopic Features
Marked diffuse fibrosis with infiltration by macrophages and eosinophils.
Remnant thyroid acini compressed by dense fibrous stroma.
Gross Appearance
“Woodlike,” stony-hard thyroid texture.
Gland often enlarged asymmetrically, firmly adherent to adjacent structures (but not skin).
Clinical Features
Neck pressure, tightness, dysphagia, hoarseness.
May have elevated thyroid autoantibodies (TPO, thyroglobulin), but often euthyroid.
TSH may be normal or slightly abnormal.
Diagnosis confirmed by thyroid biopsy.
Management
Medical Therapy: Glucocorticoids or tamoxifen can halt or reverse fibrotic progression in some cases.
Surgery: May be required for symptomatic tracheal compression.
SUBACUTE THYROIDITIS (DE QUERVAIN THYROIDITIS)
Overview
Also called subacute granulomatous thyroiditis, acute nonsuppurative thyroiditis.
Abrupt onset of hyperthyroid symptoms (fever, fatigue, myalgias), with a very tender thyroid enlargement.
Five times more frequent in women.
Pathology and Pathogenesis
Likely Viral-Related
Many have a recent history of upper respiratory infection.
Viral insult → follicular damage → release of stored T4/T3 → transient hyperthyroidism, later hypothyroid phase.
Histology
Inflammatory reaction with lymphocytes, neutrophils, necrosis of follicular cells.
Disruption of thyroid follicles.
Clinical Features
Thyroid gland is painful, tender (sometimes severely).
Enlargement often asymmetric, 1.5–2× normal size.
Pain can radiate to jaw/ears; dysphagia may occur.