Soon after the primitive cortex forms, a thin outer layer of cells (from the same mesodermal source) envelops it → permanent cortex.
By the 8th week, the forming cortex is in intimate contact with the cranial pole of the kidney and invests in a connective tissue capsule.
This early adrenal is very large compared to the kidney.
Fetal vs. Permanent Cortex
Fetal (Primitive) Cortex: Major bulk of the gland at birth; rapidly involutes after birth.
By 2 weeks postpartum, the glands lose ~1/3 of their weight.
The fetal cortex fully disappears by the end of the first year.
Permanent (Outer) Cortex: Thin at birth; differentiates further once fetal cortex involutes.
Full zonal differentiation (glomerulosa, fasciculata, reticularis) completes around the 3rd year of life.
Role of Transcription Factors
Differentiation dependent on temporal expression of genes (e.g., steroidogenic factor 1, zona glomerulosa–specific protein, inner zone antigen).
Medullary Development
Neural Crest Origin
Ectodermal cells from neural crest migrate to form sympathetic neurons (autonomic system).
Some neural crest cells differentiate into chromaffin cells instead of neurons.
Chromaffin Cells
Named for their brown staining with chromium salts (oxidation of catecholamines).
Migrate from primitive autonomic ganglia adjacent to the developing cortex into the adrenal to form the medulla (7th week onward).
Paraganglia and Organ of Zuckerkandl
Some chromaffin cells remain outside the adrenals → paraganglia along the aorta.
Organ of Zuckerkandl: A large paraganglion near the inferior mesenteric artery; prominent in fetuses, a key extra-adrenal catecholamine source in infancy.
Accessory and Absent Glands
True Accessory Adrenal Glands (cortex + medulla) are rare; can be found in celiac plexus or kidney cortex.
Adrenal “Rests” (usually cortical only) may occur near the main gland or in retroperitoneum, spleen, etc.
Gonadal Proximity during embryonic life → ectopic adrenal tissue may appear in the spermatic cord, scrotum, ovary, or broad ligament.
Absent Adrenal Gland on one side can occur but bilateral absence is extremely rare.
ANATOMY AND BLOOD SUPPLY OF THE ADRENAL GLANDS
Location and Gross Anatomy
Retroperitoneal
At the upper poles of the kidneys.
Level of ~T11 rib to L1 vertebra; each weighs ~3.5–6 g.
Capsule and Appearance
Surrounded by areolar (fatty) tissue; covered by a thin fibrous capsule.
Golden-yellow cortical tissue on section; reddish-brown medullary center.
Right Adrenal Gland
Triangular (“pyramidal”) shape.
Higher and more lateral; close to right diaphragmatic crus.
Surrounded by liver (anterosuperiorly), IVC (medially), upper pole of the right kidney (inferolaterally).
Left Adrenal Gland
Elongated or semilunar shape, slightly larger.
Often overlaps the lateral border of the aorta.
Posterior surface adjacent to diaphragm, splanchnic nerves.
Upper 2/3 behind lesser sac; lower 1/3 near pancreas body and splenic vessels.
Anatomy of the Adrenal Gland
Blood Supply
Arterial Supply: Extremely rich and variable, with 12 or more small arterial branches.
Superior Adrenal Artery (from inferior phrenic),
Middle Adrenal Artery (from aorta),
Inferior Adrenal Artery (from renal artery).
Arteries encircle the gland, forming a network to supply cortex and medulla.
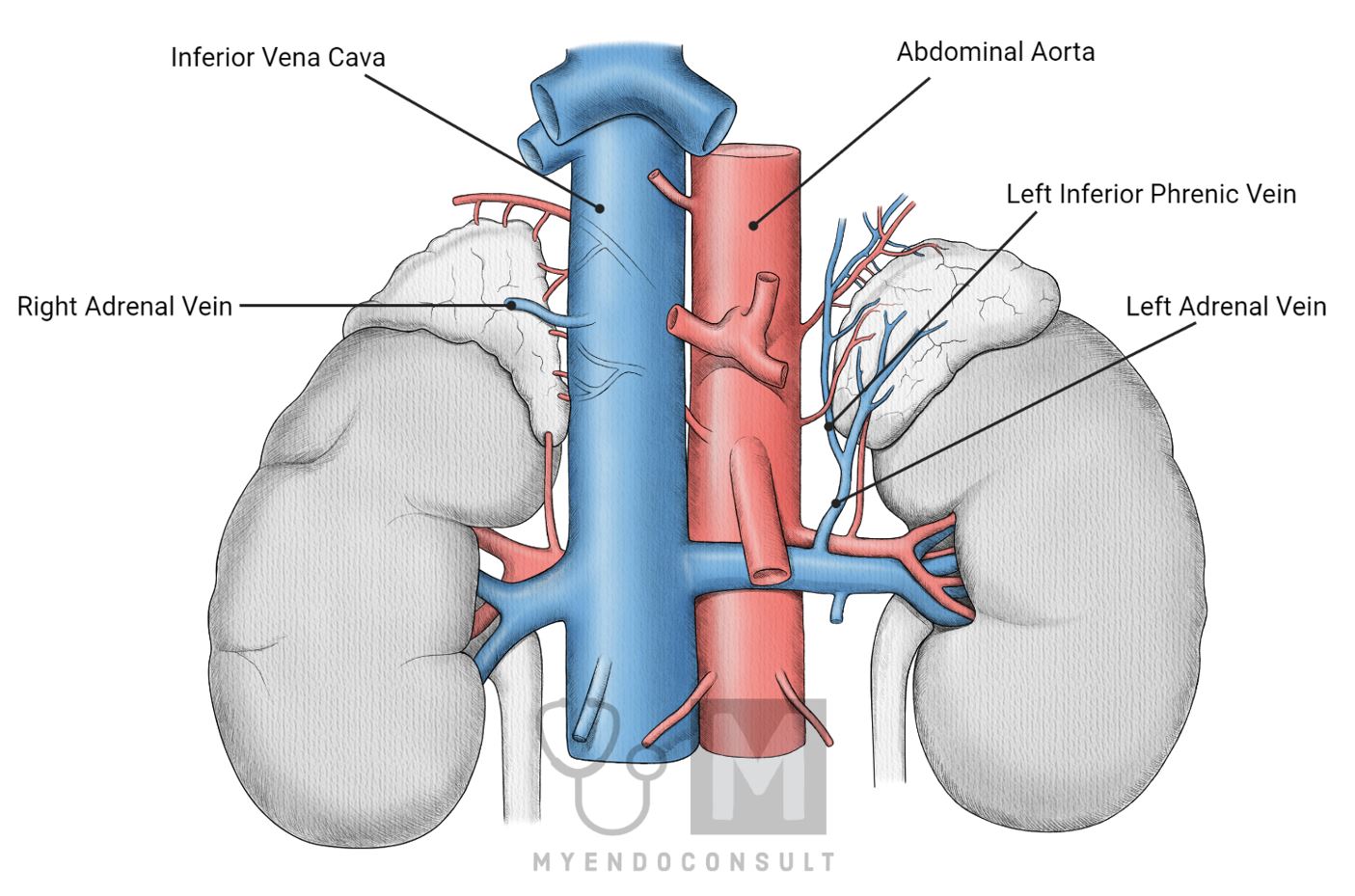
Venous Drainage
Right Adrenal Vein → directly into IVC; ~4–5 mm long.
Left Adrenal Vein → left renal vein (often joined by left inferior phrenic vein).
Both adrenals have a single large central vein that collects blood from cortex & medulla.
Adrenal Vasculature Integration
Cortical->Medullary Flow
Cortisol-rich blood from cortical sinusoids flows into medullary sinusoids.
Enhances phenylethanolamine-N-methyltransferase (PNMT) activity, converting norepinephrine to epinephrine in medulla.
Extra-adrenal chromaffin sites lack this high cortisol → produce mostly norepinephrine.
Surgical Approaches to the Adrenal Glands
Open Transabdominal
Incision: Extended subcostal or midline (for bilateral disease).
Left adrenal: via gastrocolic ligament into lesser sac → mobilize pancreas, open Gerota fascia, retract kidney.
Right adrenal: mobilize hepatic flexure, retract right liver lobe upward.
Open Posterior
Patient prone; less postoperative pain, reduced ileus.
Curvilinear incision (10th rib to iliac crest) or resection of 12th rib. Access behind kidney.
Laparoscopic Transabdominal
Standard approach for unilateral masses <8 cm with no suspicion of invasive malignancy.
Patient lateral decubitus; typically 4 trocars below costal margin.
Right side: Retract liver; left side: mobilize colonic flexure.
Lower morbidity, faster recovery.
Posterior Retroperitoneoscopic
Patient prone, 3 trocars in flank.
Insufflation of retroperitoneal space (20–25 mm Hg).
Good for patients with prior abdominal surgeries (no adhesions).
Keys to Success
Careful patient selection, knowledge of anatomy, gentle tissue handling, meticulous hemostasis, awareness of vascular anomalies.
Adrenal parenchyma is fragile.
INNERVATION OF THE ADRENAL GLANDS
Sympathetic Innervation
Preganglionic Fibers
Arise from T11–L2 spinal cord segments (lateral horns).
Travel via white rami → splanchnic nerves (greater, lesser, least) → celiac, aorticorenal, renal ganglia.
Many fibers pass through these ganglia without synapsing → form adrenal plexus on the gland’s medial border.
Medullary Innervation
Preganglionic fibers terminate directly on chromaffin cells (equivalent to postganglionic sympathetic neurons).
Some small ganglia exist within medulla or near vessels.
Parasympathetic supply from the celiac branch of posterior vagal trunk may also reach the adrenal plexus.
Functional Significance
Chromaffin Cells (in medulla) release epinephrine, norepinephrine, and dopamine.
Fight-or-Flight Response triggered by hypothalamus, pons, medulla → sympathetic outflow to T/L spine → adrenal medulla.